Resuscitation ( IF 6.5 ) Pub Date : 2022-07-21 , DOI: 10.1016/j.resuscitation.2022.07.023 A A Harhash 1 , M A Kluge 1 , A Muthukrishnan 1 , M Noc 2 , P Radsel 2 , J C Jentzer 3 , D B Seder 4 , K Lee 5 , K Lotun 5 , D Stub 6 , C-H Hsu 5 , K B Kern 5
|
Background
Recent guidelines suggest that coronary angiography (CAG) should be considered for out-of-hospital cardiac arrest (OHCA) survivors, including those without ST elevation (STE) and without shockable rhythms. However, there is no prospective data to support CAG for survivors with nonshockable rhythms and no STE post resuscitation.
Methods
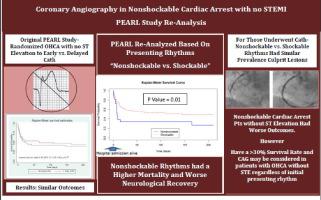
This was a re-analysis of the PEARL study (randomized OHCA survivors without STE to early CAG versus not). Patients were subdivided by initial rhythm as nonshockable (Nsh) vs shockable (Sh). The primary outcome was coronary angiographic evidence of acute culprit lesion, with secondary outcomes being survival to hospital discharge and neurological recovery.
Results
The PEARL study included 99 patients with OHCA from a presumed cardiac etiology, 24 with nonshockable and 75 with shockable rhythms. There was no difference in the frequency of CAG between the two groups [71% (Nsh) and 75% (Sh); p = 0.79], presence of CAD [81% (Nsh) and 68% (sh); p = 0.37, or culprit lesions identified in each group [50% (Nsh) and 45% (Sh); p = 0.78. Nonshockable patients had worse discharge survival [33% (Nsh) vs 57% (Sh); p = 0.04] and those survived, had worse neurological recovery [30% (Nsh) vs 54% (Sh); p = 0.02] compared to shockable patients.
Conclusions
OHCA survivors presenting with nonshockable rhythms and no STE post resuscitation had similar prevalence of culprit coronary lesions to those with shockable rhythms. CAG may be considered in patients with OHCA without STE regardless of initial presenting rhythm. There was no benefit of emergent CAG both in shockable and non-shockable rhythms.
中文翻译:
院外心脏骤停幸存者的冠状动脉造影结果,表现为非电击节律,复苏后无 ST 段抬高
背景
最近的指南建议,应考虑对院外心脏骤停 (OHCA) 幸存者进行冠状动脉造影 (CAG),包括那些没有 ST 段抬高 (STE) 和没有可电击节律的患者。然而,没有前瞻性数据支持 CAG 用于具有不可电击心律且无 STE 复苏后的幸存者。
方法
这是对 PEARL 研究的重新分析(随机 OHCA 幸存者没有 STE 到早期 CAG 与否)。患者按初始节律细分为不可电击 (Nsh) 与可电击 (Sh)。主要结果是急性罪犯病变的冠状动脉造影证据,次要结果是出院存活率和神经功能恢复。
结果
PEARL 研究包括 99 名推测为心脏病因的 OHCA 患者,其中 24 名患有不可电击的心律,75 名患有可电击的心律。两组间 CAG 的频率没有差异 [71% (Nsh) 和 75% (Sh); p = 0.79],存在 CAD [81% (Nsh) 和 68% (sh);p = 0.37,或在每组中确定的罪魁祸首病变 [50% (Nsh) 和 45% (Sh);p = 0.78。非电击患者的出院存活率更差 [33% (Nsh) vs 57% (Sh);p = 0.04],幸存者的神经恢复更差 [30% (Nsh) vs 54% (Sh);p = 0.02] 与可电击患者相比。
结论
出现不可电击节律且未进行 STE 复苏后的 OHCA 幸存者与可电击节律的患者冠状动脉病变的患病率相似。CAG 可用于无 STE 的 OHCA 患者,无论最初出现的节律如何。在可电击和不可电击的节律中,紧急 CAG 没有任何好处。

























 京公网安备 11010802027423号
京公网安备 11010802027423号