Annals of Intensive Care ( IF 8.1 ) Pub Date : 2022-07-18 , DOI: 10.1186/s13613-022-01045-1 Vincent Dupont 1, 2 , Anne-Sophie Bonnet-Lebrun 3 , Alice Boileve 4 , Julien Charpentier 5 , Jean-Paul Mira 5, 6 , Guillaume Geri 7, 8, 9 , Alain Cariou 5, 6, 10, 11, 12 , Mathieu Jozwiak 13, 14
|
Background
The optimal early mean arterial pressure (MAP) level in terms of renal function remains to be established in patients with out-of-hospital cardiac arrest (OHCA). We aimed to evaluate the association between early MAP level and severe acute kidney injury (AKI) occurrence in patients with OHCA.
Results
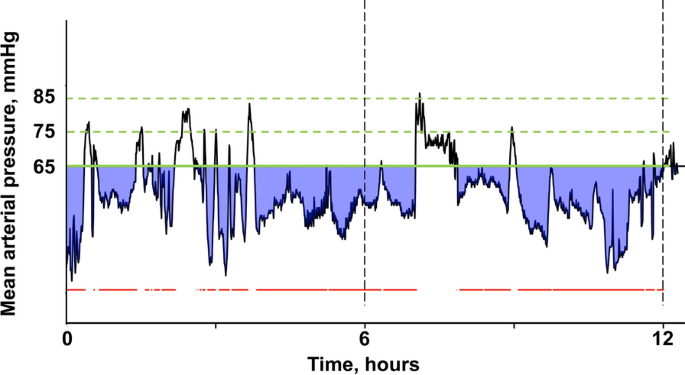
In 568 consecutive patients, the percentage time spent below a predefined MAP threshold and the corresponding area below threshold (ABT) were calculated from continuous MAP measurement. Both MAP-derived variables were calculated for different MAP thresholds (65, 75 and 85 mmHg) and time periods (the first 6 and 12 after ICU admission). 274 (48%) patients developed severe AKI defined as stage 3 of KDIGO. Both ABT and percentage time were independently associated with severe AKI, regardless of the MAP threshold and time period considered. Highest adjusted odds ratios for developing severe AKI were observed while considering the first 6 h period. Within the first 6 h, every 100 mmHg-h increase in ABT under MAP thresholds of 65, 75 and 85 mmHg increased severe AKI risk by 69% (OR = 1.69; 95% CI 1.26–2.26; p < 0.01), 13% (OR = 1.13; 95% CI 1.07–1.20; p < 0.01) and 4% (OR = 1.04; 95% CI 1.02–1.06; p < 0.01), respectively. Every 10% increase in percentage time spent under MAP thresholds of 65, 75 and 85 mmHg increased severe AKI risk by 19% (OR = 1.19; 95% CI 1.06–1.33; p < 0.01), 12% (OR = 1.12; 95% CI 1.04–1.19; p < 0.01) and 8% (OR = 1.08; 95% CI 1.02–1.14; p < 0.01), respectively.
Conclusions
Both severity and duration of early arterial hypotension after ICU admission remained associated with severe AKI occurrence while considering a MAP threshold as high as 85 mmHg after OHCA.
中文翻译:
早期平均动脉压水平对院外心脏骤停后严重急性肾损伤发生的影响
背景
院外心脏骤停 (OHCA) 患者的肾功能最佳早期平均动脉压 (MAP) 水平仍有待确定。我们旨在评估早期 MAP 水平与 OHCA 患者发生严重急性肾损伤 (AKI) 之间的关联。
结果
在 568 名连续患者中,花费在预定义 MAP 阈值以下的时间百分比和相应的阈值以下面积 (ABT) 是通过连续 MAP 测量计算的。针对不同的 MAP 阈值(65、75 和 85 mmHg)和时间段(ICU 入院后的前 6 天和第 12 天)计算了两个 MAP 衍生变量。274 名 (48%) 患者出现严重 AKI,定义为 KDIGO 的第 3 期。无论考虑的 MAP 阈值和时间段如何,ABT 和百分比时间都与严重 AKI 独立相关。在考虑前 6 小时期间,观察到发生严重 AKI 的最高调整优势比。在最初的 6 小时内,在 65、75 和 85 mmHg 的 MAP 阈值下,ABT 每增加 100 mmHg-h,严重 AKI 风险增加 69%(OR = 1.69;95% CI 1.26–2.26;p < 0.01)、13% (OR = 1.13; 95% CI 1.07–1.20; p < 0.01) 和 4% (OR = 1.04; 95% CI 1.02–1.06; p < 0.01)。在 MAP 阈值 65、75 和 85 mmHg 下花费的时间百分比每增加 10%,严重 AKI 风险就会增加 19%(OR = 1.19;95% CI 1.06–1.33;p < 0.01)、12%(OR = 1.12;95 % CI 1.04–1.19;p < 0.01) 和 8% (OR = 1.08;95% CI 1.02–1.14;p < 0.01)。
结论
考虑到 OHCA 后 MAP 阈值高达 85 mmHg,ICU 入院后早期动脉低血压的严重程度和持续时间仍然与严重 AKI 发生相关。


























 京公网安备 11010802027423号
京公网安备 11010802027423号