Journal of the American College of Cardiology ( IF 24.0 ) Pub Date : 2022-07-18 , DOI: 10.1016/j.jacc.2022.04.056 Petra Barhoum 1 , Marc Pineton de Chambrun 2 , Karim Dorgham 3 , Mathieu Kerneis 4 , Sonia Burrel 5 , Paul Quentric 6 , Christophe Parizot 3 , Juliette Chommeloux 1 , Nicolas Bréchot 1 , Quentin Moyon 7 , Guillaume Lebreton 8 , Samia Boussouar 9 , Matthieu Schmidt 10 , Hans Yssel 11 , Lucie Lefevre 1 , Makoto Miyara 3 , Jean-Luc Charuel 12 , Stéphane Marot 5 , Anne-Geneviève Marcelin 5 , Charles-Edouard Luyt 10 , Pascal Leprince 8 , Zahir Amoura 13 , Gilles Montalescot 4 , Alban Redheuil 9 , Alain Combes 10 , Guy Gorochov 3 , Guillaume Hékimian 1
|
Background
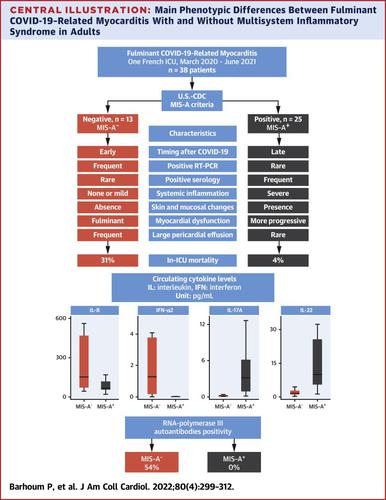
Adults who have been infected with SARS-CoV-2 can develop a multisystem inflammatory syndrome (MIS-A), including fulminant myocarditis. Yet, several patients fail to meet MIS-A criteria, suggesting the existence of distinct phenotypes in fulminant COVID-19–related myocarditis.
Objectives
This study sought to compare the characteristics and clinical outcome between patients with fulminant COVID-19–related myocarditis fulfilling MIS-A criteria (MIS-A+) or not (MIS-A−).
Methods
A monocentric retrospective analysis of consecutive fulminant COVID-19–related myocarditis in a 26-bed intensive care unit (ICU).
Results
Between March 2020 and June 2021, 38 patients required ICU admission (male 66%; mean age 32 ± 15 years) for suspected fulminant COVID-19–related myocarditis. In-ICU treatment for organ failure included dobutamine 79%, norepinephrine 60%, mechanical ventilation 50%, venoarterial extracorporeal membrane oxygenation 42%, and renal replacement therapy 29%. In-hospital mortality was 13%. Twenty-five patients (66%) met the MIS-A criteria. MIS-A− patients compared with MIS-A+ patients were characterized by a shorter delay between COVID-19 symptoms onset and myocarditis, a lower left ventricular ejection fraction, and a higher rate of in-ICU organ failure, and were more likely to require mechanical circulatory support with venoarterial extracorporeal membrane oxygenation (92% vs 16%; P < 0.0001). In-hospital mortality was higher in MIS-A− patients (31% vs 4%). MIS-A+ had higher circulating levels of interleukin (IL)-22, IL-17, and tumor necrosis factor-α (TNF-α), whereas MIS-A− had higher interferon-α2 (IFN-α2) and IL-8 levels. RNA polymerase III autoantibodies were present in 7 of 13 MIS-A− patients (54%) but in none of the MIS-A+ patients.
Conclusion
MIS-A+ and MIS-A− fulminant COVID-19–related myocarditis patients have 2 distinct phenotypes with different clinical presentations, prognosis, and immunological profiles. Differentiating these 2 phenotypes is relevant for patients’ management and further understanding of their pathophysiology.
中文翻译:
成人暴发性 COVID-19 相关心肌炎的表型异质性
背景
感染 SARS-CoV-2 的成年人可能会出现多系统炎症综合征 (MIS-A),包括暴发性心肌炎。然而,一些患者不符合 MIS-A 标准,这表明在与 COVID-19 相关的暴发性心肌炎中存在不同的表型。
目标
本研究旨在比较符合 MIS-A 标准 (MIS-A + ) 或不符合 (MIS-A - )的暴发性 COVID-19 相关心肌炎患者的特征和临床结果。
方法
对 26 个床位的重症监护病房 (ICU) 中连续暴发性 COVID-19 相关心肌炎的单中心回顾性分析。
结果
2020 年 3 月至 2021 年 6 月期间,38 名患者因疑似与 COVID-19 相关的暴发性心肌炎需要入住 ICU(男性 66%;平均年龄 32 ± 15 岁)。器官衰竭的 ICU 治疗包括多巴酚丁胺 79%、去甲肾上腺素 60%、机械通气 50%、静脉动脉体外膜氧合42% 和肾脏替代疗法 29%。住院死亡率为 13%。25 名患者 (66%) 符合 MIS-A 标准。与MIS-A+A患者的特征是 COVID-19 症状发作和心肌炎之间的延迟更短、左心室射血分数更低、ICU 内器官衰竭发生率更高,并且更有可能需要机械静脉动脉体外膜氧合的循环支持(92% 对 16%;P < 0.0001)。MIS- A患者的院内死亡率更高(31% 对 4%)。MIS-A +具有较高循环水平的白细胞介素 (IL)-22、IL-17 和肿瘤坏死因子-α (TNF-α),而 MIS-A -具有较高的干扰素-α2 (IFN-α2) 和 IL- 8个级别。RNA 聚合酶 III 自身抗体存在于 13 名 MIS-A -患者中的 7 名 (54%),但没有一名 MIS-A +患者。
结论
MIS-A +和 MIS-A -暴发性 COVID-19 相关心肌炎患者有 2 种不同的表型,具有不同的临床表现、预后和免疫学特征。区分这 2 种表型与患者的管理和进一步了解其病理生理学相关。


























 京公网安备 11010802027423号
京公网安备 11010802027423号