npj Digital Medicine ( IF 15.2 ) Pub Date : 2022-07-16 , DOI: 10.1038/s41746-022-00646-1 Jeremiah S Hinson 1, 2 , Eili Klein 1, 3 , Aria Smith 1, 2 , Matthew Toerper 1 , Trushar Dungarani 4 , David Hager 5 , Peter Hill 1 , Gabor Kelen 1 , Joshua D Niforatos 1 , R Scott Stephens 5 , Alexandra T Strauss 2, 5 , Scott Levin 1, 2
|
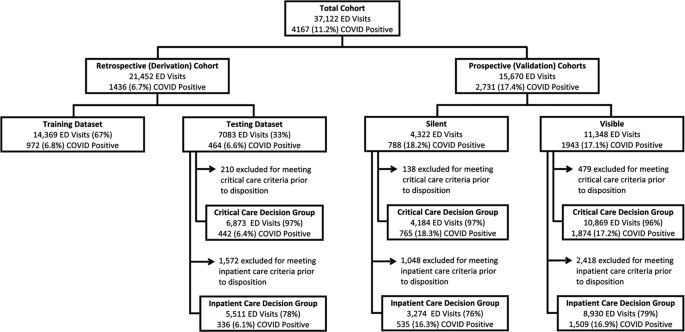
Demand has outstripped healthcare supply during the coronavirus disease 2019 (COVID-19) pandemic. Emergency departments (EDs) are tasked with distinguishing patients who require hospital resources from those who may be safely discharged to the community. The novelty and high variability of COVID-19 have made these determinations challenging. In this study, we developed, implemented and evaluated an electronic health record (EHR) embedded clinical decision support (CDS) system that leverages machine learning (ML) to estimate short-term risk for clinical deterioration in patients with or under investigation for COVID-19. The system translates model-generated risk for critical care needs within 24 h and inpatient care needs within 72 h into rapidly interpretable COVID-19 Deterioration Risk Levels made viewable within ED clinician workflow. ML models were derived in a retrospective cohort of 21,452 ED patients who visited one of five ED study sites and were prospectively validated in 15,670 ED visits that occurred before (n = 4322) or after (n = 11,348) CDS implementation; model performance and numerous patient-oriented outcomes including in-hospital mortality were measured across study periods. Incidence of critical care needs within 24 h and inpatient care needs within 72 h were 10.7% and 22.5%, respectively and were similar across study periods. ML model performance was excellent under all conditions, with AUC ranging from 0.85 to 0.91 for prediction of critical care needs and 0.80–0.90 for inpatient care needs. Total mortality was unchanged across study periods but was reduced among high-risk patients after CDS implementation.
中文翻译:
工作流集成机器学习系统的多站点实施,以优化 COVID-19 住院决策
在 2019 年冠状病毒病 (COVID-19) 大流行期间,需求已超过医疗保健供应。急诊科 (ED) 的任务是将需要医院资源的患者与可能安全出院的患者区分开来。COVID-19 的新颖性和高度可变性使这些决定具有挑战性。在这项研究中,我们开发、实施和评估了一个电子健康记录 (EHR) 嵌入式临床决策支持 (CDS) 系统,该系统利用机器学习 (ML) 来估计 COVID-19 患者或正在接受调查的患者临床恶化的短期风险。 19. 该系统将模型生成的 24 小时内重症护理需求和 72 小时内的住院护理需求转化为可快速解释的 COVID-19 恶化风险级别,在 ED 临床医生工作流程中可查看。n = 4322) 或之后 ( n = 11,348) CDS 实施;在研究期间测量了模型性能和许多以患者为导向的结果,包括住院死亡率。24 小时内重症护理需求和 72 小时内住院护理需求的发生率分别为 10.7% 和 22.5%,并且在整个研究期间相似。ML 模型在所有条件下都表现出色,预测重症监护需求的 AUC 范围为 0.85 到 0.91,住院治疗需求的 AUC 范围为 0.80-0.90。整个研究期间的总死亡率没有变化,但在实施 CDS 后高危患者的总死亡率有所降低。

























 京公网安备 11010802027423号
京公网安备 11010802027423号