Intensive Care Medicine ( IF 38.9 ) Pub Date : 2022-07-14 , DOI: 10.1007/s00134-022-06811-0 Todd A Miano 1, 2, 3 , Sean Hennessy 1, 2, 3 , Wei Yang 1, 2, 3 , Thomas G Dunn 4 , Ariel R Weisman 4 , Oluwatosin Oniyide 4 , Roseline S Agyekum 4 , Alexandra P Turner 4 , Caroline A G Ittner 4 , Brian J Anderson 4 , F Perry Wilson 5 , Raymond Townsend 6 , John P Reilly 4 , Heather M Giannini 4 , Christopher V Cosgriff 4 , Tiffanie K Jones 4 , Nuala J Meyer 4 , Michael G S Shashaty 3, 4
|
Purpose
Although dozens of studies have associated vancomycin + piperacillin–tazobactam with increased acute kidney injury (AKI) risk, it is unclear whether the association represents true injury or a pseudotoxicity characterized by isolated effects on creatinine secretion. We tested this hypothesis by contrasting changes in creatinine concentration after antibiotic initiation with changes in cystatin C concentration, a kidney biomarker unaffected by tubular secretion.
Methods
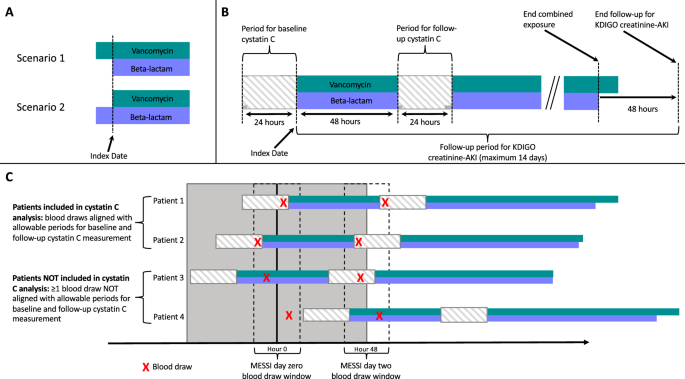
We included patients enrolled in the Molecular Epidemiology of SepsiS in the ICU (MESSI) prospective cohort who were treated for ≥ 48 h with vancomycin + piperacillin–tazobactam or vancomycin + cefepime. Kidney function biomarkers [creatinine, cystatin C, and blood urea nitrogen (BUN)] were measured before antibiotic treatment and at day two after initiation. Creatinine-defined AKI and dialysis were examined through day-14, and mortality through day-30. Inverse probability of treatment weighting was used to adjust for confounding. Multiple imputation was used to impute missing baseline covariates.
Results
The study included 739 patients (vancomycin + piperacillin–tazobactam n = 297, vancomycin + cefepime n = 442), of whom 192 had cystatin C measurements. Vancomycin + piperacillin–tazobactam was associated with a higher percentage increase of creatinine at day-two 8.04% (95% CI 1.21, 15.34) and higher incidence of creatinine-defined AKI: rate ratio (RR) 1.34 (95% CI 1.01, 1.78). In contrast, vancomycin + piperacillin–tazobactam was not associated with change in alternative biomarkers: cystatin C: − 5.63% (95% CI − 18.19, 8.86); BUN: − 4.51% (95% CI − 12.83, 4.59); or clinical outcomes: dialysis: RR 0.63 (95% CI 0.31, 1.29); mortality: RR 1.05 (95%CI 0.79, 1.41).
Conclusions
Vancomycin + piperacillin–tazobactam was associated with creatinine-defined AKI, but not changes in alternative kidney biomarkers, dialysis, or mortality, supporting the hypothesis that vancomycin + piperacillin–tazobactam effects on creatinine represent pseudotoxicity.
中文翻译:
万古霉素加哌拉西林他唑巴坦与危重症成人肌酐和胱抑素 C 早期变化的关联:一项前瞻性队列研究
目的
尽管数十项研究将万古霉素 + 哌拉西林 - 他唑巴坦与急性肾损伤 (AKI) 风险增加相关联,但尚不清楚这种关联是代表真正的损伤还是以对肌酐分泌的孤立影响为特征的假毒性。我们通过比较开始使用抗生素后肌酐浓度的变化与胱抑素 C 浓度的变化来检验这一假设,胱抑素 C 浓度是一种不受肾小管分泌影响的肾脏生物标志物。
方法
我们纳入了在 ICU (MESSI) 前瞻性队列中参加脓毒症分子流行病学研究的患者,这些患者接受了万古霉素 + 哌拉西林-他唑巴坦或万古霉素 + 头孢吡肟治疗 ≥ 48 小时。在抗生素治疗前和开始后第二天测量肾功能生物标志物 [肌酐、胱抑素 C 和血尿素氮 (BUN)]。在第 14 天检查肌酐定义的 AKI 和透析,在第 30 天检查死亡率。使用治疗加权的逆概率来调整混杂。多重插补用于插补缺失的基线协变量。
结果
该研究包括 739 名患者(万古霉素 + 哌拉西林 - 他唑巴坦n = 297,万古霉素 + 头孢吡肟n = 442),其中 192 名进行了胱抑素 C 测量。万古霉素 + 哌拉西林 - 他唑巴坦与第二天肌酐增加百分比较高 8.04%(95% CI 1.21, 15.34)和肌酐定义的 AKI 发生率较高相关:率比 (RR) 1.34 (95% CI 1.01, 1.78) ). 相比之下,万古霉素 + 哌拉西林 - 他唑巴坦与替代生物标志物的变化无关:胱抑素 C:- 5.63%(95% CI - 18.19,8.86);BUN:- 4.51% (95% CI - 12.83, 4.59);或临床结果:透析:RR 0.63 (95% CI 0.31, 1.29);死亡率:RR 1.05 (95%CI 0.79, 1.41)。
结论
万古霉素 + 哌拉西林 - 他唑巴坦与肌酐定义的 AKI 相关,但与替代肾脏生物标志物、透析或死亡率的变化无关,支持万古霉素 + 哌拉西林 - 他唑巴坦对肌酐的影响代表假毒性的假设。


























 京公网安备 11010802027423号
京公网安备 11010802027423号