American Journal of Kidney Diseases ( IF 13.2 ) Pub Date : 2022-07-09 , DOI: 10.1053/j.ajkd.2022.05.011 Debbie C Chen 1 , Michael G Shlipak 2 , Rebecca Scherzer 3 , Nisha Bansal 4 , O Alison Potok 5 , Dena E Rifkin 5 , Joachim H Ix 5 , Anthony N Muiru 1 , Chi-Yuan Hsu 6 , Michelle M Estrella 7
|
Rationale & Objective
Lower estimated glomerular filtration rate (eGFR) is associated with heart failure (HF) risk. However, eGFR based on cystatin C (eGFRcys) and creatinine (eGFRcr) may differ substantially within an individual. The clinical implications of these differences for risk of HF among persons with chronic kidney disease (CKD) are unknown.
Study Design
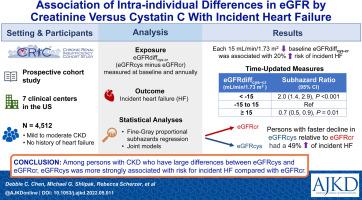
Prospective cohort study.
Setting & Participants
4,512 adults with CKD and without prevalent HF who enrolled in the Chronic Renal Insufficiency Cohort (CRIC) Study.
Exposure
Difference in GFR estimates (eGFRdiff; ie, eGFRcys minus eGFRcr).
Outcome
Incident HF hospitalization.
Analytical Approach
Fine-Gray proportional subhazards regression was used to investigate the associations of baseline, time-updated, and slope of eGFRdiff with incident HF.
Results
Of 4,512 participants, one-third had eGFRcys and eGFRcr values that differed by over 15 mL/min/1.73 m2. In multivariable-adjusted models, each 15 mL/min/1.73 m2 lower baseline eGFRdiff was associated with higher risk of incident HF hospitalization (hazard ratio [HR], 1.20 [95% CI, 1.07-1.34]). In time-updated analyses, those with eGFRdiff less than −15 mL/min/1.73 m2 had higher risk of incident HF hospitalization (HR, 1.99 [95% CI, 1.39-2.86]), and those with eGFRdiff ≥15 mL/min/1.73 m2 had lower risk of incident HF hospitalization (HR, 0.67 [95% CI, 0.49-0.91]) compared with participants with similar eGFRcys and eGFRcr. Participants with faster declines in eGFRcys relative to eGFRcr had higher risk of incident HF (HR, 1.49 [95% CI, 1.19-1.85]) compared with those in whom eGFRcys and eGFRcr declined in parallel.
Limitations
Entry into the CRIC Study was determined by eGFRcr, which constrained the range of baseline eGFRcr—but not eGFRcys—values.
Conclusions
Among persons with CKD who have large differences between eGFRcys and eGFRcr, risk for incident HF is more strongly associated with eGFRcys. Diverging slopes between eGFRcys and eGFRcr over time are also independently associated with risk of incident HF.
中文翻译:
肌酐与胱抑素 C 估计 GFR 的个体内差异与心力衰竭事件的关联
理由和目标
较低的估计肾小球滤过率 (eGFR) 与心力衰竭 (HF) 风险相关。然而,基于胱抑素 C (eGFR cys ) 和肌酐 (eGFR cr ) 的 eGFR 在个体中可能存在显着差异。这些差异对慢性肾脏病 (CKD) 患者 HF 风险的临床意义尚不清楚。
学习规划
前瞻性队列研究。
设置和参与者
4,512 名患有 CKD 但没有流行的 HF 的成年人参加了慢性肾功能不全队列 (CRIC) 研究。
接触
GFR 估计值的差异(eGFR diff;即 eGFR cys减去 eGFR cr)。
结果
事件 HF 住院。
分析方法
Fine-Gray 比例子风险回归用于研究 eGFR差异的基线、更新时间和斜率与事件 HF 的关联。
结果
在 4,512 名参与者中,三分之一的 eGFR cys和 eGFR cr值相差超过 15 mL/min/1.73 m 2。在多变量调整模型中,基线 eGFR差异每降低 15 mL/min/1.73 m 2与更高的心衰住院风险相关(风险比 [HR],1.20 [95% CI,1.07-1.34])。在时间更新分析中,eGFR diff小于 −15 mL/min/1.73 m 2的患者发生 HF 住院的风险更高(HR,1.99 [95% CI,1.39-2.86]),eGFR diff ≥15的患者与具有相似 eGFR 的参与者相比, mL/min/1.73 m 2发生 HF 住院的风险较低(HR,0.67 [95% CI,0.49-0.91])cys和 eGFR cr。与 eGFR cys和 eGFR cr平行下降的参与者相比,eGFR cys相对于 eGFR cr下降更快的参与者发生 HF 的风险更高(HR,1.49 [95% CI,1.19-1.85]) 。
限制
进入 CRIC 研究由 eGFR cr决定,它限制了基线 eGFR cr的范围——但不是 eGFR cys值。
结论
在 eGFR cys和 eGFR cr之间存在较大差异的 CKD 患者中,发生心衰的风险与 eGFR cys的相关性更强。eGFR cys和 eGFR cr之间随时间的不同斜率也与发生 HF 的风险独立相关。


























 京公网安备 11010802027423号
京公网安备 11010802027423号