Annals of Intensive Care ( IF 8.1 ) Pub Date : 2022-07-04 , DOI: 10.1186/s13613-022-01040-6 Alessandro Mele 1, 2 , Emanuele Cerminara 1, 2 , Henrike Häbel 3 , Borja Rodriguez-Galvez 4 , Anders Oldner 1, 5 , David Nelson 1, 5 , Johannes Gårdh 5 , Ragnar Thobaben 4 , Sandra Jonmarker 6, 7 , Maria Cronhjort 6, 7 , Jacob Hollenberg 8 , Johan Mårtensson 1, 5
|
Background
Whether early fluid accumulation is a risk factor for adverse renal outcomes in septic intensive care unit (ICU) patients remains uncertain. We assessed the association between cumulative fluid balance and major adverse kidney events within 30 days (MAKE30), a composite of death, dialysis, or sustained renal dysfunction, in such patients.
Methods
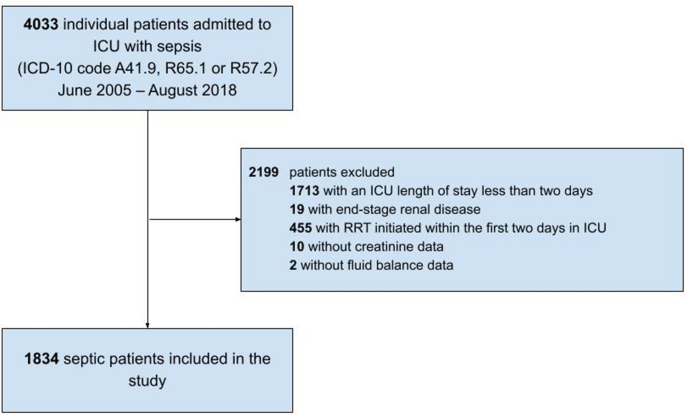
We performed a multicenter, retrospective observational study in 1834 septic patients admitted to five ICUs in three hospitals in Stockholm, Sweden. We used logistic regression analysis to assess the association between cumulative fluid balance during the first two days in ICU and subsequent risk of MAKE30, adjusted for demographic factors, comorbidities, baseline creatinine, illness severity variables, haemodynamic characteristics, chloride exposure and nephrotoxic drug exposure. We assessed the strength of significant exposure variables using a relative importance analysis.
Results
Overall, 519 (28.3%) patients developed MAKE30. Median (IQR) cumulative fluid balance was 5.3 (2.8–8.1) l in the MAKE30 group and 4.1 (1.9–6.8) l in the no MAKE30 group, with non-resuscitation fluids contributing to approximately half of total fluid input in each group. The adjusted odds ratio for MAKE30 was 1.05 (95% CI 1.02–1.09) per litre cumulative fluid balance. On relative importance analysis, the strongest factors regarding MAKE30 were, in decreasing order, baseline creatinine, cumulative fluid balance, and age. In the secondary outcome analysis, the adjusted odds ratio for dialysis or sustained renal dysfunction was 1.06 (95% CI 1.01–1.11) per litre cumulative fluid balance. On separate sensitivity analyses, lower urine output and early acute kidney injury, respectively, were independently associated with MAKE30, whereas higher fluid input was not.
Conclusions
In ICU patients with sepsis, a higher cumulative fluid balance after 2 days in ICU was associated with subsequent development of major adverse kidney events within 30 days, including death, renal replacement requirement, or persistent renal dysfunction.
中文翻译:
脓毒症中的液体积聚和主要肾脏不良事件:一项多中心观察性研究
背景
早期积液是否是脓毒症重症监护病房 (ICU) 患者肾脏不良结局的危险因素仍不确定。我们在这些患者中评估了累积体液平衡与 30 天内的主要不良肾脏事件 (MAKE30) 之间的关联,这是死亡、透析或持续肾功能不全的复合事件。
方法
我们对瑞典斯德哥尔摩三家医院的 5 个 ICU 收治的 1834 名脓毒症患者进行了一项多中心、回顾性观察研究。我们使用逻辑回归分析来评估 ICU 前两天的累积体液平衡与随后的 MAKE30 风险之间的关联,并根据人口统计学因素、合并症、基线肌酐、疾病严重程度变量、血流动力学特征、氯化物暴露和肾毒性药物暴露进行调整。我们使用相对重要性分析评估了重要暴露变量的强度。
结果
总体而言,519 名 (28.3%) 患者出现了 MAKE30。MAKE30 组中位 (IQR) 累积液体平衡为 5.3 (2.8-8.1) l,无 MAKE30 组为 4.1 (1.9-6.8) l,非复苏液体约占每组总液体输入的一半。MAKE30 的调整优势比为每升累积液体平衡 1.05 (95% CI 1.02–1.09)。在相对重要性分析中,关于 MAKE30 的最强因素依次是基线肌酐、累积体液平衡和年龄。在次要结果分析中,透析或持续肾功能不全的调整优势比为 1.06 (95% CI 1.01–1.11)/L 累积液体平衡。在单独的敏感性分析中,尿量减少和早期急性肾损伤分别与 MAKE30 独立相关,
结论
在 ICU 脓毒症患者中,ICU 2 天后较高的累积液体平衡与随后在 30 天内发生的主要不良肾脏事件相关,包括死亡、肾脏替代需要或持续性肾功能不全。


























 京公网安备 11010802027423号
京公网安备 11010802027423号