Intensive Care Medicine ( IF 38.9 ) Pub Date : 2022-07-02 , DOI: 10.1007/s00134-022-06756-4 Chiara Robba 1, 2 , Rafael Badenes 3, 4 , Denise Battaglini 1, 5 , Lorenzo Ball 1, 2 , Iole Brunetti 1 , Janus C Jakobsen 6, 7 , Gisela Lilja 8 , Hans Friberg 9 , Pedro D Wendel-Garcia 10 , Paul J Young 11, 12, 13, 14 , Glenn Eastwood 15 , Michelle S Chew 16 , Johan Unden 17, 18 , Matthew Thomas 19 , Michael Joannidis 20 , Alistair Nichol 21 , Andreas Lundin 22 , Jacob Hollenberg 23 , Naomi Hammond 24 , Manoj Saxena 25 , Martin Annborn 26 , Miroslav Solar 27, 28 , Fabio S Taccone 29 , Josef Dankiewicz 30 , Niklas Nielsen 31 , Paolo Pelosi 1, 2 ,
|
Purpose
The optimal ventilatory settings in patients after cardiac arrest and their association with outcome remain unclear. The aim of this study was to describe the ventilatory settings applied in the first 72 h of mechanical ventilation in patients after out-of-hospital cardiac arrest and their association with 6-month outcomes.
Methods
Preplanned sub-analysis of the Target Temperature Management-2 trial. Clinical outcomes were mortality and functional status (assessed by the Modified Rankin Scale) 6 months after randomization.
Results
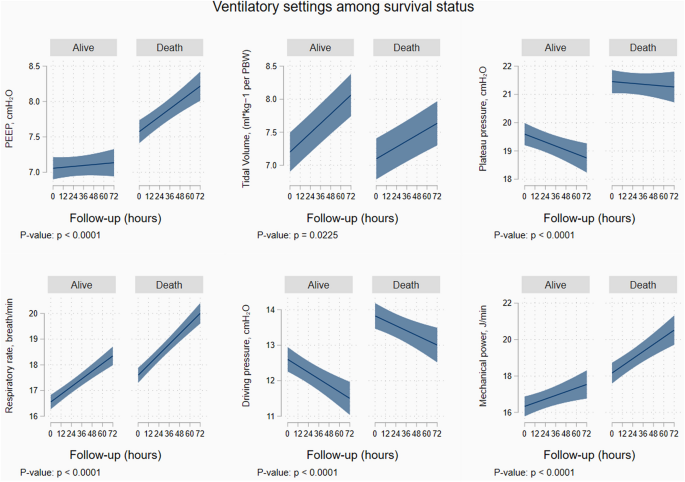
A total of 1848 patients were included (mean age 64 [Standard Deviation, SD = 14] years). At 6 months, 950 (51%) patients were alive and 898 (49%) were dead. Median tidal volume (VT) was 7 (Interquartile range, IQR = 6.2–8.5) mL per Predicted Body Weight (PBW), positive end expiratory pressure (PEEP) was 7 (IQR = 5–9) cmH20, plateau pressure was 20 cmH20 (IQR = 17–23), driving pressure was 12 cmH20 (IQR = 10–15), mechanical power 16.2 J/min (IQR = 12.1–21.8), ventilatory ratio was 1.27 (IQR = 1.04–1.6), and respiratory rate was 17 breaths/minute (IQR = 14–20). Median partial pressure of oxygen was 87 mmHg (IQR = 75–105), and partial pressure of carbon dioxide was 40.5 mmHg (IQR = 36–45.7). Respiratory rate, driving pressure, and mechanical power were independently associated with 6-month mortality (omnibus p-values for their non-linear trajectories: p < 0.0001, p = 0.026, and p = 0.029, respectively). Respiratory rate and driving pressure were also independently associated with poor neurological outcome (odds ratio, OR = 1.035, 95% confidence interval, CI = 1.003–1.068, p = 0.030, and OR = 1.005, 95% CI = 1.001–1.036, p = 0.048). A composite formula calculated as [(4*driving pressure) + respiratory rate] was independently associated with mortality and poor neurological outcome.
Conclusions
Protective ventilation strategies are commonly applied in patients after cardiac arrest. Ventilator settings in the first 72 h after hospital admission, in particular driving pressure and respiratory rate, may influence 6-month outcomes.
中文翻译:
最初 72 小时内的通气设置及其与院外心脏骤停患者结局的关联:院外心脏骤停 (TTM2) 试验后目标低温与目标常温的预先计划二次分析
目的
心脏骤停后患者的最佳通气设置及其与结果的关联仍不清楚。本研究的目的是描述在院外心脏骤停后患者机械通气的前 72 小时内应用的通气设置及其与 6 个月结局的关联。
方法
Target Temperature Management-2 试验的预先计划的子分析。临床结果是随机分组后 6 个月的死亡率和功能状态(通过改良 Rankin 量表评估)。
结果
共纳入 1848 名患者(平均年龄 64 [标准偏差,SD = 14] 岁)。6 个月时,950 名(51%)患者存活,898 名(49%)患者死亡。中位潮气量 ( VT ) 为 7(四分位距,IQR = 6.2–8.5 ) mL/预测体重 (PBW),呼气末正压 (PEEP) 为 7 (IQR = 5–9) cmH 2 0,平台压为 20 cmH 2 0 (IQR = 17–23),驱动压力为 12 cmH 20 (IQR = 10–15), 机械功率 16.2 J/min (IQR = 12.1–21.8), 通气比为 1.27 (IQR = 1.04–1.6), 呼吸频率为 17 次/分钟 (IQR = 14–20) . 中位氧分压为 87 mmHg (IQR = 75–105),二氧化碳分压为 40.5 mmHg (IQR = 36–45.7)。呼吸频率、驱动压力和机械功率与 6 个月死亡率独立相关(其非线性轨迹的综合 p 值:分别为p < 0.0001、p = 0.026 和p = 0.029)。呼吸频率和驱动压力也与不良的神经系统预后独立相关(优势比,OR = 1.035,95% 置信区间,CI = 1.003–1.068,p = 0.030,OR = 1.005,95% CI = 1.001–1.036,p = 0.048)。计算为 [(4* 驱动压力) + 呼吸频率] 的复合公式与死亡率和不良神经系统预后独立相关。
结论
保护性通气策略通常应用于心脏骤停后的患者。入院后最初 72 小时的呼吸机设置,特别是驱动压和呼吸频率,可能会影响 6 个月的结果。

























 京公网安备 11010802027423号
京公网安备 11010802027423号