Journal of the American College of Cardiology ( IF 24.0 ) Pub Date : 2022-06-20 , DOI: 10.1016/j.jacc.2022.04.021 Sameer Prasada 1 , Milind Y Desai 1 , Marwan Saad 2 , Nathaniel R Smilowitz 3 , Michael Faulx 1 , Venu Menon 1 , Rohit Moudgil 1 , Pulkit Chaudhury 1 , Ayman A Hussein 1 , Tyler Taigen 1 , Shady Nakhla 1 , Amgad Mentias 1
|
Background
The impact of pre-existing atrial fibrillation (AF) on outcomes after noncardiac surgery is not clear.
Objectives
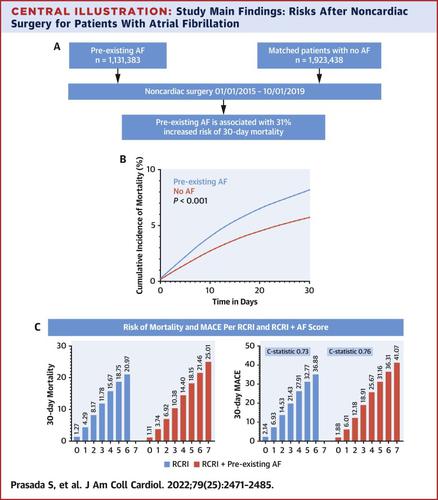
We aimed to study the impact of AF on the risk of adverse outcomes after noncardiac surgery in a nationwide cohort.
Methods
We identified Medicare beneficiaries admitted for noncardiac surgery from 2015 to 2019 and divided the study cohort into 2 groups: with and without AF. Noncardiac surgery was classified into vascular, thoracic, general, genitourinary, gynecological, orthopedics and neurosurgery, breast, head and neck, and transplant. We used propensity score matching on exact age, sex, race, urgency and type of surgery, revised cardiac risk index (RCRI) and CHA2DS2-VASc score, and tight caliper on other comorbidities. The study outcomes were 30-day mortality, stroke, myocardial infarction, and heart failure. We examined the incremental utility of AF in addition to RCRI to predict adverse events after noncardiac surgery.
Results
The study cohort included 8,635,758 patients who underwent noncardiac surgery (16.4% with AF). Patients with AF were older, more likely to be men, and had higher prevalence of comorbidities. After propensity score matching, AF was associated with higher risk of mortality (OR: 1.31; 95% CI: 1.30-1.32), heart failure (OR: 1.31; 95% CI: 1.30-1.33), and stroke (OR: 1.40; 95% CI: 1.37-1.43) and lower risk of myocardial infarction (OR: 0.81; 95% CI: 0.79-0.82). Results were consistent in subgroup analysis by sex, race, type of surgery, and all strata of RCRI and CHA2DS2-VASc score. AF improved the discriminative ability of RCRI (C-statistic 0.73 to 0.76).
Conclusion
Pre-existing AF is independently associated with postoperative adverse outcomes after NCS.
中文翻译:
非心脏手术后的术前房颤和心血管结局
背景
预先存在的心房颤动(AF) 对非心脏手术后结果的影响尚不清楚。
目标
我们的目的是在全国队列中研究 AF 对非心脏手术后不良结局风险的影响。
方法
我们确定了 2015 年至 2019 年因非心脏手术入院的医疗保险受益人,并将研究队列分为 2 组:伴有和不伴有 AF。非心脏手术分为血管外科、胸外科、普通外科、泌尿生殖外科、妇科、骨科和神经外科、乳腺、头颈部和移植。我们对确切的年龄、性别、种族、紧急程度和手术类型、修订后的心脏风险指数 (RCRI) 和 CHA 2 DS 2 -VASc 评分使用倾向评分匹配,并在其他合并症上使用卡尺。研究结果是 30 天死亡率、中风、心肌梗塞和心力衰竭。我们检查了除 RCRI 外,AF 对预测非心脏手术后不良事件的增量效用。
结果
研究队列包括 8,635,758 名接受非心脏手术的患者(16.4% 患有 AF)。房颤患者年龄较大,更可能是男性,并且合并症的发生率较高。倾向评分匹配后,房颤与较高的死亡风险(OR:1.31;95% CI:1.30-1.32)、心力衰竭(OR:1.31;95% CI:1.30-1.33)和中风(OR:1.40; 95% CI:1.37-1.43)和较低的心肌梗塞风险(OR:0.81;95% CI:0.79-0.82)。结果在按性别、种族、手术类型、RCRI 和 CHA 2 DS 2 -VASc 评分的所有层级进行的亚组分析中是一致的。AF 提高了 RCRI 的辨别能力(C 统计量 0.73 至 0.76)。
结论
预先存在的 AF 与 NCS 后的术后不良结果独立相关。

























 京公网安备 11010802027423号
京公网安备 11010802027423号