The Journal of Thoracic and Cardiovascular Surgery ( IF 6 ) Pub Date : 2022-06-15 , DOI: 10.1016/j.jtcvs.2021.01.145 Douglas R Johnston 1 , Rashed Mahboubi 2 , Edward G Soltesz 1 , Amanda S Artis 3 , Eric E Roselli 1 , Eugene H Blackstone 4 , Lars G Svensson 1 ,
|
Objectives
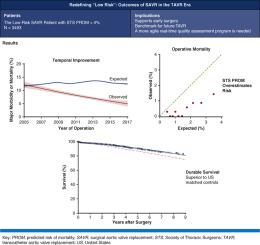
Guidelines suggest aortic valve replacement (AVR) for low-risk asymptomatic patients. Indications for transcatheter AVR now include low-risk patients, making it imperative to understand state-of-the-art surgical AVR (SAVR) in this population. Therefore, we compared SAVR outcomes in low-risk patients with those expected from Society of Thoracic Surgeons (STS) models and assessed their intermediate-term survival.
Methods
From January 2005 to January 2017, 3493 isolated SAVRs were performed in 3474 patients with STS predicted risk of mortality <4%. Observed operative mortality and composite major morbidity or mortality were compared with STS-expected outcomes according to calendar year of surgery. Logistic regression analysis was used to identify risk factors for these outcomes. Patients were followed for time-related mortality.
Results
With 15 observed operative deaths (0.43%) compared with 55 expected (1.6%), the observed:expected ratio was 0.27 for mortality (95% confidence interval [CI], 0.14-0.42), stroke 0.65 (95% CI, 0.41-0.89), and reoperation 0.50 (95% CI, 0.42-0.60). Major morbidity or mortality steadily declined, with probabilities of 8.6%, 6.7%, and 5.2% in 2006, 2011, and 2016, respectively, while STS-expected risk remained at approximately 12%. Mitral valve regurgitation, ventricular hypertrophy, pulmonary, renal, and hepatic failure, coronary artery disease, and earlier surgery date were residual risk factors. Survival was 98%, 91%, and 82% at 1, 5, and 9 years, respectively, superior to that predicted for the US age-race-sex–matched population.
Conclusions
STS risk models overestimate contemporary SAVR risk at a high-volume center, supporting efforts to create a more agile quality assessment program. SAVR in low-risk patients provides durable survival benefit, supporting early surgery and providing a benchmark for transcatheter AVR.
中文翻译:
重新定义“低风险”:经导管主动脉瓣置换时代低风险患者手术主动脉瓣置换的结果
目标
指南建议对低风险无症状患者进行主动脉瓣置换术(AVR)。经导管 AVR 的适应症现在包括低风险患者,因此必须了解这一人群中最先进的外科 AVR (SAVR)。因此,我们将低危患者的 SAVR 结果与胸外科医师协会 (STS) 模型的预期结果进行了比较,并评估了他们的中期生存率。
方法
从 2005 年 1 月到 2017 年 1 月,对 3474 名预测死亡风险 <4% 的 STS 患者进行了 3493 次单独的 SAVR。根据手术日历年,将观察到的手术死亡率和复合主要发病率或死亡率与 STS 预期结果进行比较。逻辑回归分析用于确定这些结果的风险因素。随访患者的时间相关死亡率。
结果
有 15 例观察到的手术死亡 (0.43%) 与 55 例预期 (1.6%) 相比,对于死亡率(95% 置信区间 [CI],0.14-0.42)、卒中 0.65(95% CI,0.41- 0.89),再次手术 0.50 (95% CI, 0.42-0.60)。主要发病率或死亡率稳步下降,2006 年、2011 年和 2016 年的概率分别为 8.6%、6.7% 和 5.2%,而 STS 预期风险保持在约 12%。二尖瓣反流、心室肥大、肺、肾和肝功能衰竭、冠心病和较早的手术日期是残留的危险因素。1 年、5 年和 9 年的生存率分别为 98%、91% 和 82%,优于美国年龄-种族-性别匹配人群的预测值。
结论
STS 风险模型高估了高容量中心的当代 SAVR 风险,支持创建更灵活的质量评估程序的努力。低风险患者的 SAVR 提供持久的生存益处,支持早期手术并为经导管 AVR 提供基准。

























 京公网安备 11010802027423号
京公网安备 11010802027423号