JACC: Heart Failure ( IF 13.0 ) Pub Date : 2022-06-08 , DOI: 10.1016/j.jchf.2022.03.003 Javed Butler 1 , Muhammad Shahzeb Khan 2 , JoAnn Lindenfeld 3 , William T Abraham 4 , Gianluigi Savarese 5 , Afshin Salsali 6 , Cordula Zeller 7 , Barbara Peil 8 , Gerasimos Filippatos 9 , Piotr Ponikowski 10 , Stefan D Anker 11
|
Background
Differences in clinically important thresholds in patient-reported outcomes measures such as the Kansas City Cardiomyopathy Questionnaire (KCCQ) remain less well-established in patients with heart failure with preserved ejection fraction (HFpEF) versus heart failure with reduced ejection fraction (HFrEF).
Objectives
The purpose of this study was to estimate meaningful thresholds for improvement or deterioration in the KCCQ-Total Symptom Score (TSS) in patients with HFrEF versus HFpEF.
Methods
This secondary analysis of EMPERIAL program used anchor- and distribution-based approaches to estimate thresholds for improvement or deterioration in the KCCQ-TSS using Patient Global Impression of Severity (PGIS) as the primary anchor. Mean change in KCCQ-TSS from baseline to week 12 was calculated for each PGIS.
Results
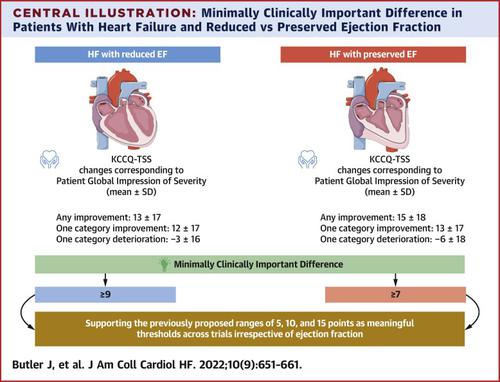
A total of 312 HFrEF and 315 HFpEF patients were enrolled. At week 12, mean changes in KCCQ-TSS corresponding to PGIS changes of “any improvement,” “1-category improvement,” and “1-category deterioration” were 13 ± 17, 12 ± 17, −3 ± 16 points in HFrEF, and 15 ± 18, 13 ± 17, −7 ± 18 points in HFpEF. Threshold for meaningful within-patient change in KCCQ-TSS was ≥9 points in HFrEF and ≥7 points in HFpEF patients. Sensitivity and specificity of ≥9 points/≥7 points change was 0.65 and 0.70 for HFrEF and 0.64 and 0.66 for HFpEF. Cumulative distribution function curves of KCCQ-TSS change from baseline to week 12 showed a shift to higher scores in both HFrEF and HFpEF patients.
Conclusions
In the EMPERIAL program, a change in KCCQ-TSS of ≥9 points in HFrEF and ≥7 points in HFpEF represents the minimal clinically important difference for improvement, confirming the broad range of 5-10 points as meaningful thresholds.
中文翻译:
HFrEF 与 HFpEF 患者健康状态评分的最小临床重要差异
背景
在射血分数保留的心力衰竭 (HFpEF) 与射血分数降低的心力衰竭 (HFrEF) 患者中,堪萨斯城心肌病问卷 (KCCQ) 等患者报告结果测量的临床重要阈值的差异仍然不太明确。
目标
本研究的目的是估计 HFrEF 与 HFpEF 患者的 KCCQ 总症状评分 (TSS) 改善或恶化的有意义阈值。
方法
对 EMPERIAL 计划的二次分析使用基于锚点和分布的方法来估计 KCCQ-TSS 改善或恶化的阈值,使用患者全球严重性印象 (PGIS) 作为主要锚点。计算每个 PGIS 的 KCCQ-TSS 从基线到第 12 周的平均变化。
结果
共招募了 312 名 HFrEF 和 315 名 HFpEF 患者。在第 12 周,HFrEF 中与“任何改善”、“1 类改善”和“1 类恶化”的 PGIS 变化相对应的 KCCQ-TSS 平均变化分别为 13 ± 17、12 ± 17、-3 ± 16 分,以及 HFpEF 中的 15 ± 18、13 ± 17、-7 ± 18 个点。KCCQ-TSS 患者内有意义的变化阈值在 HFrEF 中≥9 分,在 HFpEF 患者中≥7 分。HFrEF ≥9 点/≥7 点变化的敏感性和特异性分别为 0.65 和 0.70,HFpEF 为 0.64 和 0.66。从基线到第 12 周,KCCQ-TSS 变化的累积分布函数曲线显示 HFrEF 和 HFpEF 患者的得分都向更高的转变。
结论
在 EMPERIAL 计划中,HFrEF ≥9 分和 HFpEF ≥7 分的 KCCQ-TSS 变化代表改善的最小临床重要差异,确认 5-10 分的广泛范围是有意义的阈值。

























 京公网安备 11010802027423号
京公网安备 11010802027423号