Clinical Pharmacokinetics ( IF 4.5 ) Pub Date : 2022-06-08 , DOI: 10.1007/s40262-022-01140-3 Shweta Urva 1 , Tonya Quinlan 1 , John Landry 1 , Xiaosu Ma 1 , Jennifer A Martin 1 , Charles T Benson 1
|
Background and Objective
Tirzepatide, a novel, once-weekly, dual glucose-dependent insulinotropic polypeptide and glucagon-like peptide-1 receptor agonist, is approved in the US as a treatment for type 2 diabetes and is under development for long-term weight management, heart failure with preserved ejection fraction, and nonalcoholic steatohepatitis. This study evaluated the pharmacokinetics and tolerability of tirzepatide in participants with hepatic impairment (with or without type 2 diabetes) versus healthy participants with normal hepatic function.
Methods
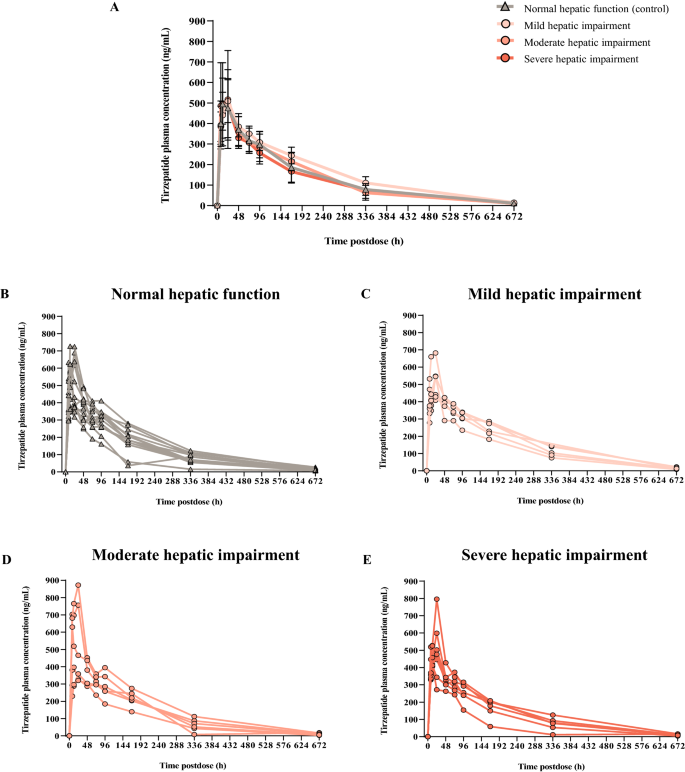
Participants in this parallel, single-dose, open-label study were categorized by hepatic impairment defined by the baseline Child-Pugh (CP) score A (mild impairment; n = 6), B (moderate impairment; n = 6), or C (severe impairment; n = 7) or normal hepatic function (n = 13). All participants received a single subcutaneous 5-mg dose of tirzepatide. Blood samples were collected to determine tirzepatide plasma concentrations to estimate pharmacokinetic parameters. The primary pharmacokinetic parameters of area under the drug concentration–time curve from zero to infinity (AUC0–∞) and maximum observed drug concentration (Cmax) were evaluated using an analysis of covariance. The geometric least-squares means (LSM) and mean ratios for each group, between control and hepatic impairment levels, and the corresponding 90% confidence intervals (CIs) were estimated. The analysis of the time to maximum observed drug concentration was based on a nonparametric method. The relationships between the pharmacokinetic parameters and CP classification parameters (serum albumin level, total bilirubin level, and international normalized ratio) were also assessed. Adverse events were monitored to assess safety and tolerability.
Results
Tirzepatide exposure, based on AUC0–∞ and Cmax, was similar across the control and hepatic impairment groups. Statistical analysis showed no difference in the geometric LSM AUC0–∞ or Cmax between participants in the control group and the hepatic impairment groups, with the 90% CI for the ratios of geometric LSM spanning unity (AUC0–∞ ratio of geometric LSM vs control [90% CI 1.08 [0.879, 1.32], 0.960 [0.790, 1.17], and 0.852 [0.699, 1.04] and Cmax ratio of geometric LSM vs control [90% CI]: 0.916 [0.726, 1.16], 1.00 [0.802, 1.25], and 0.972 [0.784, 1.21] for mild, moderate and severe hepatic impairment groups, respectively). There was no change in median time to Cmax of tirzepatide across all groups (time to Cmax median difference vs control [90% CI]: 0 [− 4.00, 12.00], 0 [− 12.00, 12.00], and 0 [− 11.83, 4.17], respectively). There was no significant relationship between the exposure of tirzepatide and the CP score (p > 0.1 for AUC0–∞, Cmax, and apparent total body clearance). Similarly, there was no clinically relevant relationship between the exposure of tirzepatide and serum albumin level, total bilirubin level, or international normalized ratio. The geometric LSM half-life values were also similar across the control and hepatic impairment groups. No notable differences in safety profiles were observed between participants with hepatic impairment and healthy control participants.
Conclusions
Tirzepatide pharmacokinetics was similar in participants with varying degrees of hepatic impairment compared with healthy participants. Thus, people with hepatic impairment treated with tirzepatide may not require dose adjustments.
Clinical Trial Registration
ClinicalTrials.gov identifier number NCT03940742.
中文翻译:
肝功能损害对双 GIP 和 GLP-1 受体激动剂替西帕肽药代动力学的影响
背景与目的
Tirzepatide 是一种新型、每周一次、双重葡萄糖依赖性促胰岛素多肽和胰高血糖素样肽-1 受体激动剂,在美国被批准用于治疗 2 型糖尿病,并且正在开发用于长期体重管理、心力衰竭保留射血分数和非酒精性脂肪性肝炎。本研究评估了替西帕肽在肝功能损害(伴或不伴 2 型糖尿病)参与者与肝功能正常的健康参与者中的药代动力学和耐受性。
方法
这项平行、单剂量、开放标签研究的参与者按由基线 Child-Pugh (CP) 评分 A(轻度损伤;n = 6)、B(中度损伤;n = 6)或C(严重受损;n = 7)或肝功能正常(n = 13)。所有参与者都接受了单次皮下 5 mg 剂量的 tirzepatide。收集血样以确定替西帕肽血浆浓度以估计药代动力学参数。从零到无穷大的药物浓度-时间曲线下面积(AUC 0-∞ )和最大观察药物浓度(Cmax )的主要药代动力学参数) 使用协方差分析进行评估。估计了每组的几何最小二乘均值 (LSM) 和平均比率,在控制和肝损伤水平之间,以及相应的 90% 置信区间 (CI)。达到最大观察到的药物浓度的时间分析基于非参数方法。还评估了药代动力学参数和 CP 分类参数(血清白蛋白水平、总胆红素水平和国际标准化比率)之间的关系。监测不良事件以评估安全性和耐受性。
结果
基于 AUC 0-∞和C max的 Tirzepatide 暴露在对照组和肝损伤组中相似。统计分析显示,对照组和肝损伤组参与者的几何 LSM AUC 0-∞或C max没有差异,几何 LSM 的比率跨越统一(几何 LSM 的 AUC 0-∞比率)的 90% CI与对照 [90% CI 1.08 [0.879, 1.32]、0.960 [0.790, 1.17] 和 0.852 [0.699, 1.04] 和C max几何 LSM 与对照组的比率 [90% CI]:轻度、中度和重度肝损伤组分别为 0.916 [0.726, 1.16]、1.00 [0.802, 1.25] 和 0.972 [0.784, 1.21])。在所有组中,tirzepatide达到C max的中位时间没有变化(至C max中位差异与对照的时间 [90% CI]:0 [- 4.00, 12.00]、0 [- 12.00, 12.00] 和 0 [- 11.83, 4.17],分别)。替西帕肽的暴露量与 CP 评分之间没有显着相关性(对于 AUC 0-∞,p > 0.1 , C max和明显的全身清除率)。同样,替西帕肽的暴露量与血清白蛋白水平、总胆红素水平或国际标准化比率之间没有临床相关关系。对照组和肝损伤组的几何 LSM 半衰期值也相似。在肝功能损害的参与者和健康对照参与者之间没有观察到安全性方面的显着差异。
结论
与健康参与者相比,不同程度肝功能损害的参与者的 Tirzepatide 药代动力学相似。因此,用替西帕肽治疗的肝功能不全患者可能不需要调整剂量。
临床试验注册
ClinicalTrials.gov 标识符号 NCT03940742。
























 京公网安备 11010802027423号
京公网安备 11010802027423号