JACC: Cardiovascular Imaging ( IF 14.0 ) Pub Date : 2022-01-12 , DOI: 10.1016/j.jcmg.2021.11.009 Aniek L van Wijngaarden 1 , Valentina Mantegazza 2 , Yasmine L Hiemstra 1 , Valentina Volpato 2 , Pieter van der Bijl 1 , Mauro Pepi 2 , Meindert Palmen 3 , Victoria Delgado 1 , Nina Ajmone Marsan 1 , Gloria Tamborini 2 , Jeroen J Bax 1
|
Background
In patients with severe primary mitral regurgitation (MR), the indication for surgery is currently based on the presence of symptoms, left ventricular dilatation and dysfunction, atrial fibrillation, and pulmonary hypertension.
Objectives
The aim of this study was to evaluate the prognostic impact of the presence of extra–mitral valve cardiac involvement (including known risk factors but also severe left atrial [LA] dilatation and right ventricular [RV] dysfunction) in a large multicenter study of patients with primary MR.
Methods
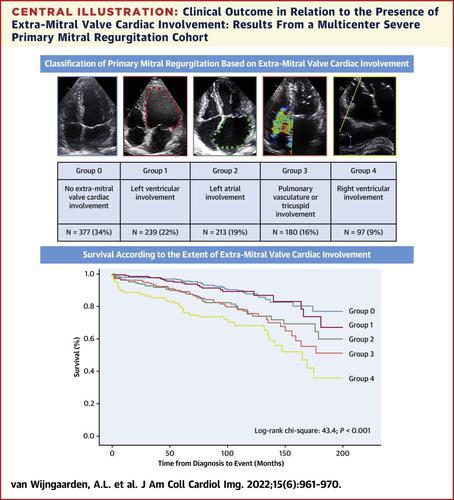
Patients with severe primary MR undergoing surgery were included and categorized according to the extent (highest) of cardiac involvement: group 0, no cardiac involvement; group 1, left ventricular involvement; group 2, LA involvement; group 3, pulmonary vasculature or tricuspid valve involvement; or group 4, RV involvement. The outcome was all-cause mortality.
Results
A total of 1,106 patients were included (mean age 63 ± 12 years, 68% male). In total, 377 patients (34%) were classified in group 0, 239 (22%) in group 1, 213 (19%) in group 2, 180 (16%) in group 3, and 97 (9%) in group 4. Kaplan-Meier curve analysis revealed significantly worse survival (log-rank chi-square = 43.4; P < 0.001) with higher group. On multivariable analysis, age, male sex, chronic obstructive pulmonary disease, kidney function, and group of cardiac involvement were independently associated with all-cause mortality. For each increase in group, a 17% higher risk for all-cause mortality was observed (95% CI: 1.051-1.313; P = 0.005) during a median follow-up time of 88 months.
Conclusions
In patients with severe primary MR, a novel classification system based on extra–mitral valve cardiac involvement may help refine risk stratification and timing of surgery, particularly including severe LA dilatation and RV dysfunction in the assessment.
中文翻译:
二尖瓣外心脏受累对原发性二尖瓣关闭不全患者的预后影响
背景
对于重度原发性二尖瓣关闭不全 (MR) 患者,手术指征目前基于是否存在症状、左心室扩张和功能障碍、心房颤动和肺动脉高压。
目标
本研究的目的是在一项针对患者的大型多中心研究中评估二尖瓣外心脏受累(包括已知的危险因素,但也包括严重的左心房 [LA] 扩张和右心室 [RV] 功能障碍)对预后的影响与原发性 MR。
方法
接受手术的严重原发性 MR 患者被纳入并根据心脏受累程度(最高)进行分类:0 组,无心脏受累;第 1 组,左心室受累;第 2 组,LA 参与;第 3 组,肺血管系统或三尖瓣受累;或第 4 组,RV 受累。结果是全因死亡率。
结果
共纳入 1,106 名患者(平均年龄 63 ± 12 岁,68% 为男性)。总共有 377 名患者(34%)被归入第 0 组,239 名(22%)患者被归入第 1 组,213 名(19%)患者被归入第 2 组,180 名(16%)患者被归入第 3 组,97 名患者(9%)被归入第 1 组4. Kaplan-Meier 曲线分析显示,较高组的生存率显着降低(对数秩卡方 = 43.4;P < 0.001)。在多变量分析中,年龄、男性、慢性阻塞性肺疾病、肾功能和心脏受累组与全因死亡率独立相关。在88 个月的中位随访时间内,每组增加 17% 的全因死亡率风险(95% CI:1.051-1.313;P = 0.005)。
结论
在重度原发性 MR 患者中,基于二尖瓣外心脏受累的新分类系统可能有助于改进风险分层和手术时机,特别是在评估中包括重度 LA 扩张和 RV 功能障碍。


























 京公网安备 11010802027423号
京公网安备 11010802027423号