JACC: Cardiovascular Imaging ( IF 14.0 ) Pub Date : 2022-01-12 , DOI: 10.1016/j.jcmg.2021.11.027 Jorge Corral Acero 1 , Andreas Schuster 2 , Ernesto Zacur 1 , Torben Lange 2 , Thomas Stiermaier 3 , Sören J Backhaus 2 , Holger Thiele 4 , Alfonso Bueno-Orovio 5 , Pablo Lamata 6 , Ingo Eitel 3 , Vicente Grau 1
|
Background
Left ventricular ejection fraction (LVEF) and end-systolic volume (ESV) remain the main imaging biomarkers for post-acute myocardial infarction (AMI) risk stratification. However, they are limited to global systolic function and fail to capture functional and anatomical regional abnormalities, hindering their performance in risk stratification.
Objectives
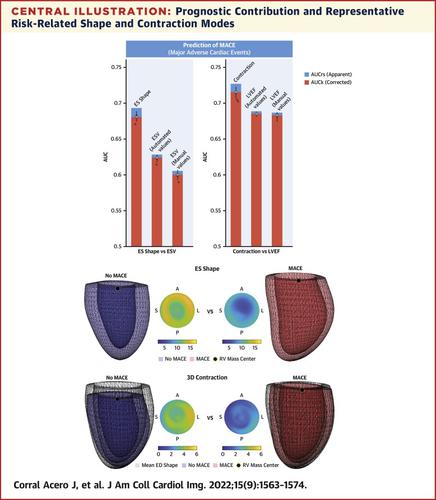
This study aimed to identify novel 3-dimensional (3D) imaging end-systolic (ES) shape and contraction descriptors toward risk-related features and superior prognosis in AMI.
Methods
A multicenter cohort of AMI survivors (n = 1,021; median age 63 years; 74.5% male) who underwent cardiac magnetic resonance (CMR) at a median of 3 days after infarction were considered for this study. The clinical endpoint was the 12-month rate of major adverse cardiac events (MACE; n = 73), consisting of all-cause death, reinfarction, and new congestive heart failure. A fully automated pipeline was developed to segment CMR images, build 3D statistical models of shape and contraction in AMI, and find the 3D patterns related to MACE occurrence.
Results
The novel ES shape markers proved to be superior to ESV (median cross-validated area under the receiver-operating characteristic curve 0.681 [IQR: 0.679-0.684] vs 0.600 [IQR: 0.598-0.602]; P < 0.001); and 3D contraction to LVEF (0.716 [IQR: 0.714-0.718] vs 0.681 [IQR: 0.679-0.684]; P < 0.001) in MACE occurrence prediction. They also contributed to a significant improvement in a multivariable setting including CMR markers, cardiovascular risk factors, and basic patient characteristics (0.747 [IQR: 0.745-0.749]; P < 0.001). Based on these novel 3D descriptors, 3 impairments caused by AMI were identified: global, anterior, and basal, the latter being the most complementary signature to already known predictors.
Conclusions
The quantification of 3D differences in ES shape and contraction, enabled by a fully automated pipeline, improves post-AMI risk prediction and identifies shape and contraction patterns related to MACE occurrence.
中文翻译:
使用自动左心室形状分析了解和改进心肌梗死后的风险评估
背景
左心室射血分数 (LVEF) 和收缩末期容积 (ESV) 仍然是急性心肌梗死后 (AMI) 风险分层的主要影像生物标志物。然而,它们仅限于整体收缩功能,无法捕获功能和解剖区域异常,阻碍了它们在风险分层中的表现。
目标
本研究旨在确定新的 3 维 (3D) 成像收缩末期 (ES) 形状和收缩描述符,以实现 AMI 的风险相关特征和良好预后。
方法
本研究考虑了在梗塞后中位 3 天接受心脏磁共振 (CMR) 的多中心 AMI 幸存者队列(n = 1,021;中位年龄 63 岁;74.5% 为男性)。临床终点是 12 个月的主要不良心脏事件(MACE;n = 73)发生率,包括全因死亡、再梗死和新发充血性心力衰竭。开发了一个全自动管道来分割 CMR 图像,构建 AMI 中形状和收缩的 3D 统计模型,并找到与 MACE 发生相关的 3D 模式。
结果
新型 ES 形状标记被证明优于 ESV(接受者操作特征曲线下的中值交叉验证面积 0.681 [IQR:0.679-0.684] 对比 0.600 [IQR:0.598-0.602];P < 0.001 );在 MACE 发生预测中,3D 收缩对 LVEF(0.716 [IQR:0.714-0.718] vs 0.681 [IQR:0.679-0.684];P < 0.001)。它们还有助于显着改善多变量设置,包括 CMR 标志物、心血管危险因素和基本患者特征 (0.747 [IQR:0.745-0.749];P < 0.001)。基于这些新颖的 3D 描述符,确定了由 AMI 引起的 3 种损伤:全局、前部和基底,后者是已知预测因子的最互补特征。
结论
通过全自动管道实现的 ES 形状和收缩的 3D 差异量化,改进了 AMI 后风险预测,并识别与 MACE 发生相关的形状和收缩模式。


























 京公网安备 11010802027423号
京公网安备 11010802027423号