JACC: Cardiovascular Imaging ( IF 14.0 ) Pub Date : 2021-11-17 , DOI: 10.1016/j.jcmg.2021.09.017 C Charles Jain 1 , Juerg Tschirren 2 , Yogesh N V Reddy 1 , Vojtech Melenovsky 3 , Margaret Redfield 1 , Barry A Borlaug 1
|
Objectives
The authors hypothesized that quantitative computed tomography (QCT) imaging would reveal subclinical increases in lung congestion in patients with heart failure and preserved ejection fraction (HFpEF) and that this would be related to pulmonary vascular hemodynamic abnormalities.
Background
Gross evidence of lung congestion on physical examination, laboratory tests, and radiography is typically absent among compensated ambulatory patients with HFpEF. However, pulmonary gas transfer abnormalities are commonly observed and associated with poor outcomes.
Methods
Patients referred for invasive hemodynamic exercise testing who had undergone chest computed tomography imaging within 1 month were identified (N = 137). A novel artificial intelligence QCT algorithm was used to measure pulmonary fluid content.
Results
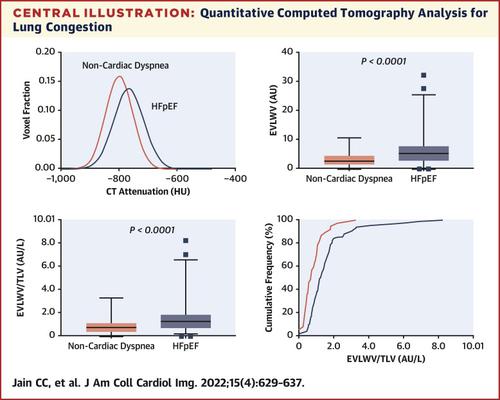
Compared with control subjects with noncardiac dyspnea, patients with HFpEF displayed increased mean lung density (–758 HU [–793, –709 HU] vs –787 HU [–828, –747 HU]; P = 0.002) and a higher ratio of extravascular lung water to total lung volume (EVLWV/TLV) (1.25 [0.80, 1.76] vs 0.66 [0.01, 1.03]; P < 0.0001) by QCT imaging, indicating greater lung congestion. EVLWV/TLV was directly correlated with pulmonary vascular pressures at rest, with stronger correlations observed during exercise. Patients with increasing tertiles of EVLWV/TLV demonstrated higher mean pulmonary artery pressures at rest (34 ± 11 mm Hg vs 39 ± 14 mm Hg vs 45 ± 17 mm Hg; P = 0.0003) and during exercise (55 ± 17 mm Hg vs 59 ± 17 mm Hg vs 69 ± 22 mm Hg; P = 0.0003).
Conclusions
QCT imaging identifies subclinical lung congestion in HFpEF that is not clinically apparent but is related to abnormalities in pulmonary vascular hemodynamics. These data provide new insight into the long-term effects of altered hemodynamics on pulmonary structure and function in HFpEF.
中文翻译:
射血分数保留型心力衰竭的亚临床肺充血和血流动力学异常
目标
作者假设定量计算机断层扫描 (QCT) 成像将揭示心力衰竭和射血分数正常 (HFpEF) 患者肺充血的亚临床增加,这与肺血管血流动力学异常有关。
背景
在代偿性门诊 HFpEF 患者中,通常没有体格检查、实验室检查和放射学检查显示肺充血的总体证据。然而,肺部气体传输异常很常见,并且与不良预后相关。
方法
确定了在 1 个月内接受过胸部计算机断层扫描成像的有创血流动力学运动测试患者 (N = 137)。一种新的人工智能 QCT 算法被用来测量肺液含量。
结果
与非心源性呼吸困难的对照受试者相比,HFpEF 患者的平均肺密度增加(–758 HU [–793, –709 HU] 对比 –787 HU [–828, –747 HU];P = 0.002)和更高的QCT 成像显示血管外肺水占肺总容积 (EVLWV/TLV)(1.25 [0.80, 1.76] vs 0.66 [0.01, 1.03];P < 0.0001),表明肺充血程度更高。EVLWV/TLV 与静息时的肺血管压力直接相关,在运动期间观察到更强的相关性。EVLWV/TLV 三分位数增加的患者在静息时(34 ± 11 mm Hg 对 39 ± 14 mm Hg 对 45 ± 17 mm Hg; P = 0.0003)和运动期间(55 ± 17 mm Hg 对 59)表现出更高的平均肺动脉压± 17 毫米汞柱与 69 ± 22 毫米汞柱;P =0.0003)。
结论
QCT 成像可识别 HFpEF 的亚临床肺充血,这种充血在临床上并不明显,但与肺血管血流动力学异常有关。这些数据为了解血流动力学改变对 HFpEF 肺结构和功能的长期影响提供了新的见解。


























 京公网安备 11010802027423号
京公网安备 11010802027423号