JACC: Cardiovascular Interventions ( IF 11.3 ) Pub Date : 2021-10-27 , DOI: 10.1016/j.jcin.2021.08.037 Afik Snir 1 , Michael K Wilson 2 , Lining A Ju 3 , Yunduo Zhao 3 , Sophia Wong 2 , Lynn Khor 4 , Christopher Naoum 2 , Kirby Wong 5 , Anthony Keech 6 , David S Celermajer 6 , Martin K Ng 1
|
Objectives
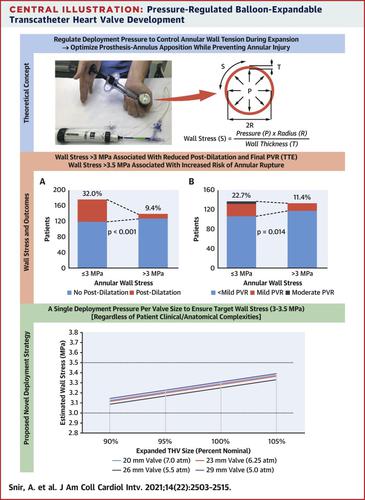
The authors propose a novel pressure-regulated method for balloon-expandable transcatheter heart valve (THV) deployment, aimed at optimizing prosthesis-annulus apposition while preventing significant tissue injury.
Background
The optimal method for balloon-expandable THV deployment remains debated. Current protocols are volume dependent, relying on under- and overfilling of the deployment apparatus. During deployment, the annular wall tension exerted by the expanding prosthesis is determined by maximal THV diameter and balloon pressure (Laplace’s law).
Methods
Three hundred thirty consecutive patients with severe native aortic stenosis who underwent TAVR with SAPIEN 3 THVs were included. One hundred and six patients were considered at high risk for annular rupture. THVs were deployed until reaching a predetermined balloon pressure. Postdilatation was performed to reduce mild or greater angiographic paravalvular regurgitation (PVR). Using a biomechanical model, annular wall stress was estimated for each case and assessed against rates of postdilatation, mild or greater PVR on transthoracic echocardiography, new permanent pacemaker placement or left bundle branch block, and annular rupture.
Results
Patients with wall stress >3 MPa had reduced postdilatation rate (P < 0.001) and reduced final PVR (P = 0.014). Annular rupture occurred in 2 of 3 high-risk patients with wall stress >3.5 MPa (3.69 and 3.84 MPa); no rupture occurred in 95 high-risk patients with wall stress ≤3.5 MPa. We defined a single target deployment pressure per THV size to ensure deployment within target wall stress levels of 3 to 3.5 MPa: 6.25 atm for 23-mm THVs, 5.5 atm for 26-mm THVs, and 5 atm for 29-mm THVs. Patients within this target range (n = 136) had a 10.0% postdilatation rate, 12.7% mild PVR, and no moderate to severe PVR. The relationship between balloon filling volume and associated pressure and wall stress was inconsistent.
Conclusions
Pressure-regulated THV deployment is a simple, reproducible, safe, and effective method, regardless of high-risk anatomical complexities.
中文翻译:
提高球囊扩张式经导管主动脉瓣安全性和有效性的新型压力调节部署策略
目标
作者提出了一种用于球囊扩张式经导管心脏瓣膜 (THV) 部署的新型压力调节方法,旨在优化假体与瓣环的结合,同时防止严重的组织损伤。
背景
球囊可扩展 THV 部署的最佳方法仍然存在争议。当前的协议依赖于体积,依赖于部署装置的不足和过度填充。在展开期间,由扩张假体施加的环形壁张力由最大 THV 直径和球囊压力(拉普拉斯定律)决定。
方法
包括 330 名连续接受 SAPIEN 3 THV 的 TAVR 的严重自体主动脉瓣狭窄患者。106 名患者被认为是环状破裂的高风险。部署 THV 直到达到预定的球囊压力。进行后扩张以减少轻度或更大的血管造影瓣周返流(PVR)。使用生物力学模型,估计每个病例的环壁应力,并评估后扩张率、经胸超声心动图轻度或更大的 PVR、新的永久性起搏器放置或左束支传导阻滞和环破裂。
结果
壁应力>3 MPa 的患者后扩张率降低(P < 0.001),最终 PVR 降低(P = 0.014)。3 名高危患者中有 2 名发生了瓣环破裂,管壁应力 >3.5 MPa(3.69 和 3.84 MPa);95例壁应力≤3.5 MPa的高危患者均未发生破裂。我们为每个 THV 尺寸定义了单个目标部署压力,以确保在 3 至 3.5 MPa 的目标壁应力水平内部署:23-mm THV 为 6.25 atm,26-mm THV 为 5.5 atm,29-mm THV 为 5 atm。此目标范围内的患者 (n = 136) 的后扩张率为 10.0%,轻度 PVR 为 12.7%,且无中度至重度 PVR。球囊充盈量与相关压力和壁应力之间的关系不一致。
结论
压力调节的 THV 部署是一种简单、可重复、安全且有效的方法,无论高风险的解剖复杂性如何。

























 京公网安备 11010802027423号
京公网安备 11010802027423号