International Journal of Cardiology ( IF 3.5 ) Pub Date : 2021-10-25 , DOI: 10.1016/j.ijcard.2021.10.136 Salaheldin Ahmed 1 , Abdulla Ahmed 1 , Göran Rådegran 1
|
Background
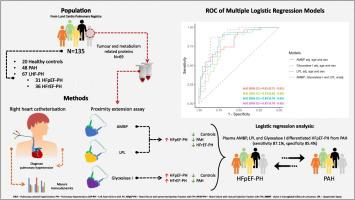
Discrimination of heart failure with preserved ejection fraction with pulmonary hypertension (HFpEF-PH) from pulmonary arterial hypertension (PAH) is crucial for clinical management but may be challenging due to similarities in clinical and comorbid characteristics. We aimed to investigate tumour and metabolism related proteins in differentiating HFpEF-PH from PAH.
Methods
Sixty-nine tumour and metabolism plasma proteins were analysed with proximity extension assay in heathy controls (n = 20), patients with PAH (n = 48) and LHF-PH (n = 67) [HFpEF-PH (n = 31) and HF reduced EF-PH (n = 36)]. Haemodynamics were assessed with right heart catheterization.
Results
The plasma levels of alpha-1-microglobulin/bikunin precursor (AMBP) and lipoprotein lipase (LPL), were higher in HFpEF-PH compared to healthy controls (p < 0.01), HFrEF-PH (p < 0.05), and PAH (p < 0.001). Glyoxalase I levels were higher in HFpEF-PH and HFrEF-PH compared to controls (p < 0.001) and PAH (p < 0.001). Each of plasma AMBP, LPL, and glyoxalase I, adjusted for age and sex in multivariable logistic regression models, could differentiate HFpEF-PH from PAH, with areas under the receiver operating characteristic curve (AUC) of 0.81, 0.84 and 0.79, respectively. The combination of AMBP, LPL and glyoxalse I yielded the largest AUC of 0.87 [95% confidence interval (0.79–0.95)] in discriminating HFpEF-PH from PAH, with a sensitivity of 87.1% and a specificity of 85.4%. In HFpEF-PH, the plasma levels of AMBP correlated with pulmonary arterial wedge pressure (rs = −0.42, p = 0.018).
Conclusions
Plasma AMBP, LPL and glyoxalase I may facilitate the distinction of HFpEF-PH from PAH. Larger clinical studies are encouraged to confirm and validate our findings.
中文翻译:
血浆肿瘤和代谢相关的生物标志物 AMBP、LPL 和乙二醛酶 I 区分射血分数保留的心力衰竭伴肺动脉高压和肺动脉高压
背景
区分肺动脉高压 (HFpEF-PH) 与肺动脉高压 (PAH) 的心力衰竭对临床管理至关重要,但由于临床和合并症特征的相似性,可能具有挑战性。我们旨在研究肿瘤和代谢相关蛋白在区分 HFpEF-PH 和 PAH 中的作用。
方法
在健康对照组 ( n = 20)、PAH ( n = 48) 和 LHF-PH ( n = 67) [HFpEF-PH ( n = 31) 和HF 降低 EF-PH ( n = 36)]。用右心导管术评估血流动力学。
结果
与健康对照组(p < 0.01)、HFrEF-PH(p < 0.05)和 PAH(p < 0.001)。与对照组相比,HFpEF-PH 和 HFrEF-PH 中的乙二醛酶 I 水平更高(p < 0.001) 和 PAH (p < 0.001)。血浆 AMBP、LPL 和乙二醛酶 I 中的每一个,在多变量逻辑回归模型中针对年龄和性别进行调整后,都可以区分 HFpEF-PH 和 PAH,受试者工作特征曲线下面积 (AUC) 分别为 0.81、0.84 和 0.79。AMBP、LPL 和乙二醛 I 的组合在区分 HFpEF-PH 和 PAH 方面产生的最大 AUC 为 0.87 [95% 置信区间 (0.79–0.95)],灵敏度为 87.1%,特异性为 85.4%。在 HFpEF-PH 中,AMBP的血浆水平与肺动脉楔压相关(rs = -0.42,p = 0.018)。
结论
血浆 AMBP、LPL 和乙二醛酶 I 可能有助于区分 HFpEF-PH 和 PAH。鼓励进行更大规模的临床研究来确认和验证我们的发现。

























 京公网安备 11010802027423号
京公网安备 11010802027423号