JACC: Cardiovascular Interventions ( IF 11.3 ) Pub Date : 2021-09-20 , DOI: 10.1016/j.jcin.2021.07.015 Vinayak N Bapat 1 , Syed Zaid 2 , Shinichi Fukuhara 3 , Shekhar Saha 4 , Keti Vitanova 5 , Philipp Kiefer 6 , John J Squiers 7 , Pierre Voisine 8 , Luigi Pirelli 9 , Moritz Wyler von Ballmoos 10 , Michael W A Chu 11 , Josep Rodés-Cabau 8 , J Michael DiMaio 7 , Michael A Borger 6 , Rudiger Lange 5 , Christian Hagl 4 , Paolo Denti 12 , Thomas Modine 13 , Tsuyoshi Kaneko 14 , Gilbert H L Tang 15 ,
|
Objectives
The aim of this study was to evaluate clinical characteristics, mechanisms of failure, and outcomes of transcatheter aortic valve replacement (TAVR) explantation.
Background
Surgical explantation following TAVR may be required for structural valve degeneration, paravalvular leak, infection, or other reasons. However, in-depth data on indications and outcomes are lacking.
Methods
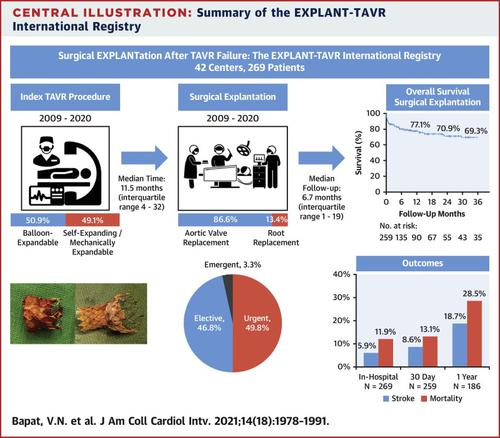
Data from a multicenter, international registry (EXPLANT-TAVR) of patients who underwent TAVR explantation were reviewed retrospectively. Explantations performed during the same admission as initial TAVR were excluded. Clinical and echocardiographic outcomes were evaluated. Median follow-up duration was 6.7 months (interquartile range [IQR]: 1.0-18.8 months) after TAVR explantation and was 97.7% complete at 30 days and 86.1% complete at 1 year.
Results
From November 2009 to September 2020, 269 patients across 42 centers with a mean age of 72.7 ± 10.4 years underwent TAVR explantation. About one quarter (25.9%) were deemed low surgical risk at index TAVR, and median Society of Thoracic Surgeons risk at TAVR explantation was 5.6% (IQR: 3.2%-9.6%). The median time to explantation was 11.5 months (IQR: 4.0-32.4 months). Balloon-expandable and self-expanding or mechanically expandable valves accounted for 50.9% and 49.1%, respectively. Indications for explantation included endocarditis (43.1%), structural valve degeneration (20.1%), paravalvular leak (18.2%), and prosthesis-patient mismatch (10.8%). Redo TAVR was not feasible because of unfavorable anatomy in 26.8% of patients. Urgent or emergency cases were performed in 53.1% of patients, aortic root replacement in 13.4%, and 54.6% had concomitant cardiac procedures. Overall survival at last follow-up was 76.1%. In-hospital, 30-day, and 1-year mortality rates were 11.9%, 13.1%, and 28.5%, respectively, and stroke rates were 5.9%, 8.6%, and 18.7%, respectively.
Conclusions
The EXPLANT-TAVR registry reveals that surgical risks associated with TAVR explantation are not negligible and should be taken into consideration in the lifetime management of aortic stenosis.
中文翻译:
TAVR 失败后的手术切除
目标
本研究的目的是评估经导管主动脉瓣置换术 (TAVR) 移植的临床特征、失败机制和结果。
背景
由于结构性瓣膜变性、瓣周漏、感染或其他原因,可能需要在 TAVR 后进行手术切除。然而,缺乏关于适应症和结果的深入数据。
方法
对接受 TAVR 移植的患者的多中心国际注册 (EXPLANT-TAVR) 的数据进行了回顾性审查。在与初始 TAVR 相同的入院期间进行的移植被排除在外。评估了临床和超声心动图结果。TAVR 外植后中位随访时间为 6.7 个月(四分位距 [IQR]:1.0-18.8 个月),30 天完成 97.7%,1 年完成 86.1%。
结果
从 2009 年 11 月到 2020 年 9 月,来自 42 个中心的 269 名平均年龄为 72.7 ± 10.4 岁的患者接受了 TAVR 外植。大约四分之一 (25.9%) 的 TAVR 指数被认为是低手术风险,TAVR 外植体的中位风险为 5.6%(IQR:3.2%-9.6%)。外植的中位时间为 11.5 个月(IQR:4.0-32.4 个月)。球囊扩张型和自扩张型或机械扩张型瓣膜分别占 50.9% 和 49.1%。移植指征包括心内膜炎(43.1%)、结构性瓣膜变性(20.1%)、瓣周漏(18.2%)和假体-患者不匹配(10.8%)。由于 26.8% 的患者解剖结构不利,重做 TAVR 不可行。53.1% 的患者进行了紧急或急诊手术,13.4% 和 54% 的患者进行了主动脉根部置换术。6% 有伴随的心脏手术。最后一次随访时的总生存率为 76.1%。住院、30 天和 1 年死亡率分别为 11.9%、13.1% 和 28.5%,卒中率分别为 5.9%、8.6% 和 18.7%。
结论
EXPLANT-TAVR 登记显示,与 TAVR 移植相关的手术风险不可忽略,应在主动脉瓣狭窄的终生管理中予以考虑。
























 京公网安备 11010802027423号
京公网安备 11010802027423号