The Journal of Thoracic and Cardiovascular Surgery ( IF 6 ) Pub Date : 2021-09-17 , DOI: 10.1016/j.jtcvs.2021.09.016 Masaaki Sato 1 , Masashi Kobayashi 2 , Jin Sakamoto 3 , Ryuta Fukai 4 , Hiromitsu Takizawa 5 , Shinji Shinohara 6 , Fumitsugu Kojima 7 , Akira Sakurada 8 , Jun Nakajima 1
|
Objectives
Virtual-assisted lung mapping 2.0 is a novel preoperative bronchoscopic lung mapping technique combining the multiple dye marks of conventional virtual-assisted lung mapping with intrabronchial microcoils to navigate thoracoscopic deep lung resection. This study's purpose was to evaluate the feasibility of virtual-assisted lung mapping 2.0 in resecting deeply located pulmonary nodules with adequate margins.
Methods
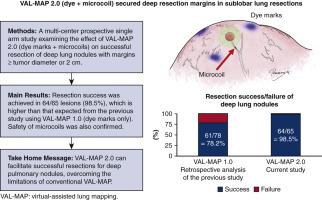
A multicenter, prospective single-arm study was performed from 2019 to 2020 in 8 institutions. The selection criteria were barely identifiable nodules requiring sublobar lung resections, nodules requiring resection lines reaching the inner 2/3 of the pulmonary lobe on computed tomography images in wedge resection, or the nodule center located in the inner 2/3 of the pulmonary lobe in wedge resection or segmentectomy. Resection margins larger than 2 cm or the nodule diameter were considered successful resection. Bronchoscopic placement of multiple dye marks and microcoil(s) was conducted 0 to 2 days before surgery.
Results
We analyzed 65 lesions in 64 patients. The diameter and depth of the targeted nodules and the minimum required resection depth reported as median (interquartile range) were 9 (7-13) mm, 11 (5-15) mm, and 30 (25-35) mm, respectively. Among 60 wedge resections and 5 segmentectomies, successful resection was achieved in 64 of 65 resections (98.5%; 95% confidence interval, 91.7-100). Among 75 microcoils placed, 3 showed major displacement after bronchoscopic placement. There were no severe adverse events associated with the virtual-assisted lung mapping procedure.
Conclusions
This study demonstrated that virtual-assisted lung mapping 2.0 can facilitate successful resections for deep pulmonary nodules, overcoming the limitations of conventional virtual-assisted lung mapping.
中文翻译:
虚拟辅助肺标测2.0结合微线圈和染料标记在肺深部切除中的作用
目标
虚拟辅助肺标测 2.0 是一种新颖的术前支气管镜肺标测技术,将传统虚拟辅助肺标测的多个染料标记与支气管内微线圈相结合,以导航胸腔镜深部肺切除术。本研究的目的是评估虚拟辅助肺标测 2.0 在切除具有足够边缘的深部肺结节方面的可行性。
方法
2019 年至 2020 年在 8 个机构中进行了一项多中心、前瞻性单臂研究。选择标准是几乎无法识别的结节需要亚肺叶切除,在楔形切除术中,在计算机断层扫描图像上需要切除线到达肺叶内 2/3 的结节,或者在肺叶内 2/3 内的结节中心。楔形切除术或肺段切除术。切除边缘大于 2 cm 或结节直径被认为是成功切除。在手术前 0 至 2 天进行支气管镜下放置多个染料标记和微线圈。
结果
我们分析了 64 名患者的 65 个病灶。靶向结节的直径和深度以及报告为中位数(四分位距)的最小所需切除深度分别为 9 (7-13) mm、11 (5-15) mm 和 30 (25-35) mm。在 60 次楔形切除和 5 次节段切除中,65 次切除中有 64 次成功切除(98.5%;95% 置信区间,91.7-100)。在放置的 75 个微线圈中,3 个在支气管镜下放置后出现严重移位。没有与虚拟辅助肺标测程序相关的严重不良事件。
结论
这项研究表明,虚拟辅助肺标测 2.0 可以促进深部肺结节的成功切除,克服了传统虚拟辅助肺标测的局限性。

























 京公网安备 11010802027423号
京公网安备 11010802027423号