The Journal of Thoracic and Cardiovascular Surgery ( IF 6 ) Pub Date : 2021-09-14 , DOI: 10.1016/j.jtcvs.2021.09.010 Chin Siang Ong 1 , Erik Reinertsen 2 , Haoqi Sun 3 , Philicia Moonsamy 1 , Navyatha Mohan 1 , Masaki Funamoto 1 , Tsuyoshi Kaneko 4 , Prem S Shekar 4 , Stefano Schena 5 , Jennifer S Lawton 5 , David A D'Alessandro 1 , M Brandon Westover 6 , Aaron D Aguirre 7 , Thoralf M Sundt 1
|
Objective
Current cardiac surgery risk models do not address a substantial fraction of procedures. We sought to create models to predict the risk of operative mortality for an expanded set of cases.
Methods
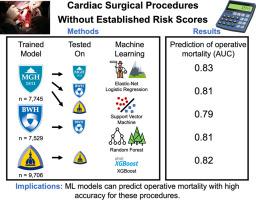
Four supervised machine learning models were trained using preoperative variables present in the Society of Thoracic Surgeons (STS) data set of the Massachusetts General Hospital to predict and classify operative mortality in procedures without STS risk scores. A total of 424 (5.5%) mortality events occurred out of 7745 cases. Models included logistic regression with elastic net regularization (LogReg), support vector machine, random forest (RF), and extreme gradient boosted trees (XGBoost). Model discrimination was assessed via area under the receiver operating characteristic curve (AUC), and calibration was assessed via calibration slope and expected-to-observed event ratio. External validation was performed using STS data sets from Brigham and Women's Hospital (BWH) and the Johns Hopkins Hospital (JHH).
Results
Models performed comparably with the highest mean AUC of 0.83 (RF) and expected-to-observed event ratio of 1.00. On external validation, the AUC was 0.81 in BWH (RF) and 0.79 in JHH (LogReg/RF). Models trained and applied on the same institution's data achieved AUCs of 0.81 (BWH: LogReg/RF/XGBoost) and 0.82 (JHH: LogReg/RF/XGBoost).
Conclusions
Machine learning models trained on preoperative patient data can predict operative mortality at a high level of accuracy for cardiac surgical procedures without established risk scores. Such procedures comprise 23% of all cardiac surgical procedures nationwide. This work also highlights the value of using local institutional data to train new prediction models that account for institution-specific practices.
中文翻译:
预测未确定风险评分的心脏外科手术患者的手术死亡率
客观的
目前的心脏手术风险模型没有解决很大一部分手术。我们试图创建模型来预测更多病例的手术死亡率风险。
方法
使用马萨诸塞州综合医院胸外科医师协会 (STS) 数据集中存在的术前变量对四个监督机器学习模型进行训练,以预测和分类没有 STS 风险评分的手术中的手术死亡率。在 7745 例病例中,共有 424 例 (5.5%) 发生死亡事件。模型包括具有弹性网络正则化 (LogReg) 的逻辑回归、支持向量机、随机森林 (RF) 和极端梯度增强树 (XGBoost)。通过接受者操作特征曲线 (AUC) 下的面积评估模型辨别力,并通过校准斜率和预期观察事件比评估校准。使用来自布莱根妇女医院 (BWH) 和约翰霍普金斯医院 (JHH) 的 STS 数据集进行外部验证。
结果
模型的表现与最高平均 AUC 0.83 (RF) 和预期与观察到的事件比率 1.00 相当。在外部验证中,AUC 在 BWH (RF) 中为 0.81,在 JHH (LogReg/RF) 中为 0.79。在同一机构的数据上训练和应用的模型实现了 0.81(BWH:LogReg/RF/XGBoost)和 0.82(JHH:LogReg/RF/XGBoost)的 AUC。
结论
根据术前患者数据训练的机器学习模型可以在没有确定风险评分的情况下以高精度预测心脏外科手术的手术死亡率。此类手术占全国所有心脏外科手术的 23%。这项工作还强调了使用本地机构数据来训练新的预测模型以说明机构特定实践的价值。

























 京公网安备 11010802027423号
京公网安备 11010802027423号