Heart Rhythm ( IF 5.5 ) Pub Date : 2021-09-03 , DOI: 10.1016/j.hrthm.2021.08.033 Parikshit S Sharma 1 , Neil R Patel 2 , Venkatesh Ravi 1 , Dipen V Zalavadia 3 , Sujitraj Dommaraju 2 , Varun Garg 1 , Timothy R Larsen 1 , Angela M Naperkowski 3 , Jeremiah Wasserlauf 1 , Kousik Krishnan 1 , Wilson Young 4 , Parash Pokharel 5 , Jess W Oren 5 , Randle H Storm 5 , Richard G Trohman 1 , Henry D Huang 1 , Faiz A Subzposh 3 , Pugazhendhi Vijayaraman 3
|
Background
Left bundle branch area pacing (LBBAP) has been shown to be a feasible option for patients requiring ventricular pacing.
Objective
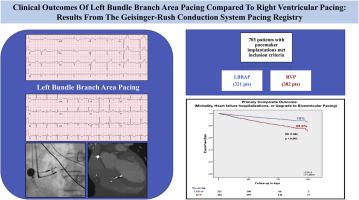
The purpose of this study was to compare clinical outcomes between LBBAP and RVP among patients undergoing pacemaker implantation
Methods
This observational registry included patients who underwent pacemaker implantations with LBBAP or RVP for bradycardia indications between April 2018 and October 2020. The primary composite outcome included all-cause mortality, heart failure hospitalization (HFH), or upgrade to biventricular pacing. Secondary outcomes included the composite endpoint among patients with a prespecified burden of ventricular pacing and individual outcomes.
Results
A total of 703 patients met inclusion criteria (321 LBBAP and 382 RVP). QRS duration during LBBAP was similar to baseline (121 ± 23 ms vs 117 ± 30 ms; P = .302) and was narrower compared to RVP (121 ± 23 ms vs 156 ± 27 ms; P <.001). The primary composite outcome was significantly lower with LBBAP (10.0%) compared to RVP (23.3%) (hazard ratio [HR] 0.46; 95%T confidence interval [CI] 0.306–0.695; P <.001). Among patients with ventricular pacing burden >20%, LBBAP was associated with significant reduction in the primary outcome compared to RVP (8.4% vs 26.1%; HR 0.32; 95% CI 0.187–0.540; P <.001). LBBAP was also associated with significant reduction in mortality (7.8% vs 15%; HR 0.59; P = .03) and HFH (3.7% vs 10.5%; HR 0.38; P = .004).
Conclusion
LBBAP resulted in improved clinical outcomes compared to RVP. Higher burden of ventricular pacing (>20%) was the primary driver of these outcome differences.
中文翻译:
与右心室起搏相比,左束支区起搏的临床结果:来自 Geisinger-Rush 传导系统起搏登记处的结果
背景
左束支区起搏 (LBBAP) 已被证明是需要心室起搏患者的可行选择。
客观的
本研究的目的是比较 LBBAP 和 RVP 在接受起搏器植入患者中的临床结果
方法
该观察性登记包括在 2018 年 4 月至 2020 年 10 月期间因心动过缓适应症接受 LBBAP 或 RVP 起搏器植入的患者。主要复合结果包括全因死亡率、心力衰竭住院 (HFH) 或升级为双心室起搏。次要结果包括具有预先指定的心室起搏负担的患者的复合终点和个体结果。
结果
共有 703 名患者符合纳入标准(321 名 LBBAP 和 382 名 RVP)。LBBAP 期间的 QRS 持续时间与基线相似(121 ± 23 ms 对比 117 ± 30 ms;P = .302)并且与 RVP 相比更窄(121 ± 23 ms 对比 156 ± 27 ms;P <.001)。与 RVP (23.3%) 相比,LBBAP (10.0%) 的主要复合结果显着降低(风险比 [HR] 0.46;95%T 置信区间 [CI] 0.306–0.695;P <.001 )。在心室起搏负荷 >20% 的患者中,与 RVP 相比,LBBAP 与主要结果的显着降低相关(8.4% 对 26.1%;HR 0.32;95% CI 0.187–0.540;P <.001 )。LBBAP 还与死亡率显着降低相关(7.8% 对 15%;HR 0.59;P= .03) 和 HFH(3.7% 对 10.5%;HR 0.38;P = .004)。
结论
与 RVP 相比,LBBAP 可改善临床结果。较高的心室起搏负担 (>20%) 是这些结果差异的主要驱动因素。


























 京公网安备 11010802027423号
京公网安备 11010802027423号