Resuscitation ( IF 6.5 ) Pub Date : 2021-08-23 , DOI: 10.1016/j.resuscitation.2021.08.026 Ahmed A Harhash 1 , Teresa May 2 , Chiu-Hsieh Hsu 3 , David B Seder 2 , Josef Dankiewicz 4 , Sachin Agarwal 5 , Nainesh Patel 6 , John McPherson 7 , Richard Riker 2 , Eldar Soreide 8 , Karen G Hirsch 9 , Pascal Stammet 10 , Allison Dupont 11 , Sune Forsberg 12 , Sten Rubertsson 13 , Hans Friberg 4 , Niklas Nielsen 14 , Michael R Mooney 15 , Karl B Kern 16
|
Background
Out of Hospital Cardiac arrest (OHCA) survivors with ST elevation (STE) with or without shockable rhythms often benefit from coronary angiography (CAG) and, if indicated, percutaneous coronary intervention (PCI). However, the benefits of CAG and PCI in OHCA survivors with nonshockable rhythms (PEA/asystole) and no STE are debated.
Methods
Using the International Cardiac Arrest Registry (INTCAR 2.0), representing 44 centers in the US and Europe, comatose OHCA survivors with known presenting rhythms and post resuscitation ECGs were identified. Survival to hospital discharge, neurological recovery on discharge, and impact of CAG with or without PCI on such outcome were assessed and compared with other groups (shockable rhythms with or without STE).
Results
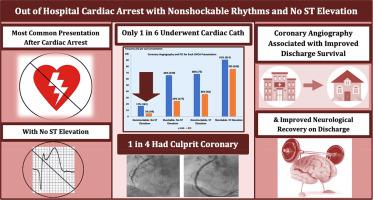
Total of 2113 OHCA survivors were identified and described as; nonshockable/no STE (Nsh-NST) (n = 940, 44.5%), shockable/no STE (Sh-NST) (n = 716, 33.9%), nonshockable/STE (Nsh-ST) (n = 110, 5.2%), and shockable/STE (Sh-ST) (n = 347, 16.4%). Of Nsh-NST, 13.7% (129) were previously healthy before CA and only 17.3% (161) underwent CAG; of those, 30.4% (52) underwent PCI. A total of 18.6% (174) Nsh-NST patients survived to hospital discharge, with 57.5% (100) of such survivors having good neurological recovery (cerebral performance category 1 or 2) on discharge. Coronary angiography was associated with improved odds for survival and neurological recovery among all groups, including those with NSh-NST.
Conclusions
Nonshockable initial rhythms with no ST elevation post resuscitation was the most common presentation after OHCA. Although most of these patients did not undergo coronary angiography, among those who did, 1 in 4 patients had a culprit lesion and underwent revascularization. Invasive CAG should be at least considered for all OHCA survivors, including those with nonshockable rhythms and no ST elevation post resuscitation.
Brief abstract
Out of hospital cardiac arrest (OHCA) survivors with ST elevation and/or shockable rhythms benefit from coronary angiography and revascularization. Nonshockable cardiac arrest survivors with no ST elevation have the worst prognosis and rarely undergo coronary angiography.
Nonshockable rhythms with no ST elevation was the most common presentation after OHCA and among a small subgroup underwent coronary angiography, 1 in 4 patients with had culprit lesion and underwent revascularization. Coronary angiography was associated with high prevalence of acute culprit coronary lesions and should be considered for those with a probably cardiac cause for their arres.
中文翻译:
具有非电击初始节律且复苏后无 ST 段抬高的患者的心脏干预发生率和相关的心脏骤停结果
背景
具有或不具有可电击节律的 ST 段抬高 (STE) 的院外心脏骤停 (OHCA) 幸存者通常受益于冠状动脉造影 (CAG),如果有指征,经皮冠状动脉介入治疗 (PCI)。然而,CAG 和 PCI 对非电击心律(PEA/心搏停止)且无 STE 的 OHCA 幸存者的益处存在争议。
方法
使用代表美国和欧洲 44 个中心的国际心脏骤停登记处 (INTCAR 2.0),确定了具有已知呈现节律和复苏后心电图的昏迷 OHCA 幸存者。评估出院存活率、出院时神经功能恢复以及 CAG 有或没有 PCI 对此类结果的影响,并与其他组(有或没有 STE 的可电击节律)进行比较。
结果
共有 2113 名 OHCA 幸存者被确定并描述为:不可电击/无 STE (Nsh-NST) (n = 940, 44.5%),可电击/无 STE (Sh-NST) (n = 716, 33.9%),不可电击/STE (Nsh-ST) (n = 110, 5.2 %) 和可电击/STE (Sh-ST)(n = 347, 16.4%)。在 Nsh-NST 中,13.7% (129) 在 CA 之前是健康的,只有 17.3% (161) 接受了 CAG;其中,30.4% (52) 接受了 PCI。共有 18.6% (174) Nsh-NST 患者存活至出院,其中 57.5% (100) 的此类幸存者在出院时具有良好的神经功能恢复(大脑表现类别 1 或 2)。冠状动脉造影与所有组(包括 NSh-NST 组)的生存率和神经功能恢复的几率提高有关。
结论
OHCA 后最常见的表现是复苏后无 ST 段抬高的非电击初始节律。尽管这些患者中的大多数没有接受冠状动脉造影,但在那些接受了冠状动脉造影的患者中,四分之一的患者有罪魁祸首病变并接受了血运重建术。至少应考虑对所有 OHCA 幸存者进行侵入性 CAG,包括那些具有不可电击节律且复苏后无 ST 段抬高的患者。
摘要
具有 ST 段抬高和/或可电击节律的院外心脏骤停 (OHCA) 幸存者受益于冠状动脉造影和血运重建。无 ST 段抬高的非电击心脏骤停幸存者预后最差,很少接受冠状动脉造影。
无 ST 段抬高的非电击节律是 OHCA 后最常见的表现,在一小部分接受冠状动脉造影的患者中,四分之一的患者有罪犯病变并接受了血运重建。冠状动脉造影与急性罪犯冠状动脉病变的高患病率有关,对于可能是心脏原因导致心搏骤停的患者,应考虑进行冠状动脉造影。

























 京公网安备 11010802027423号
京公网安备 11010802027423号