Hepatology International ( IF 6.6 ) Pub Date : 2021-05-11 , DOI: 10.1007/s12072-021-10188-5 Yang Yang 1 , Sirui Fu 1 , Bin Cao 2 , Kenan Hao 3 , Yong Li 1 , Jianwen Huang 1 , Wenfeng Shi 4 , Chongyang Duan 5 , Xiao Bai 1 , Kai Tang 1 , Shirui Yang 6 , Xiaofeng He 3 , Ligong Lu 1
|
Background/purpose
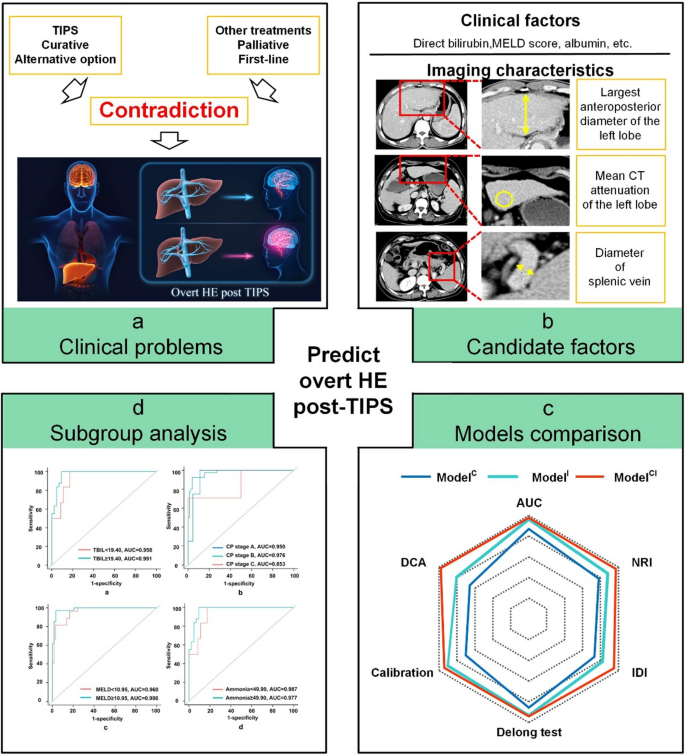
Overt hepatic encephalopathy (HE) risk should be preoperatively predicted to identify patients suitable for curative transjugular intrahepatic portosystemic shunt (TIPS) instead of palliative treatments.
Methods
A total of 185 patients who underwent TIPS procedure were randomised (130 in the training dataset and 55 in the validation dataset). Clinical factors and imaging characteristics were assessed. Three different models were established by logistic regression analyses based on clinical factors (ModelC), imaging characteristics (ModelI), and a combination of both (ModelCI). Their discrimination, calibration, and decision curves were compared, to identify the best model. Subgroup analysis was performed for the best model.
Results
ModelCI, which contained two clinical factors and two imaging characteristics, was identified as the best model. The areas under the curve of ModelC, ModelI, and ModelCI were 0.870, 0.963, and 0.978 for the training dataset and 0.831, 0.971, and 0.969 for the validation dataset. The combined model outperformed the clinical and imaging models in terms of calibration and decision curves. The performance of ModelCI was not influenced by total bilirubin, Child–Pugh stages, model of end-stage liver disease score, or ammonia. The subgroup with a risk score ≥ 0.88 exhibited a higher proportion of overt HE (training dataset: 13.3% vs. 97.4%, p < 0.001; validation dataset: 0.0% vs. 87.5%, p < 0.001).
Conclusion
Our combination model can successfully predict the risk of overt HE post-TIPS. For the low-risk subgroup, TIPS can be performed safely; however, for the high-risk subgroup, it should be considered more carefully.
Graphic abstract
中文翻译:
经颈静脉肝内门体分流术治疗后明显肝性脑病的预测:一项队列研究
背景/目的
应在术前预测明显的肝性脑病 (HE) 风险,以确定适合治愈性经颈静脉肝内门体分流术 (TIPS) 而非姑息治疗的患者。
方法
共有 185 名接受 TIPS 手术的患者被随机分组(训练数据集中 130 名,验证数据集中 55 名)。评估临床因素和影像学特征。基于临床因素(模型C)、影像学特征(模型I)以及两者的组合(模型CI),通过逻辑回归分析建立了三种不同的模型。比较它们的鉴别、校准和决策曲线,以确定最佳模型。对最佳模型进行亚组分析。
结果
包含两个临床因素和两个影像特征的模型CI被确定为最佳模型。模型C、模型I和模型CI的曲线下面积对于训练数据集为 0.870、0.963 和 0.978,对于验证数据集为 0.831、0.971 和 0.969。组合模型在校准和决策曲线方面优于临床和成像模型。模型CI的性能不受总胆红素、Child-Pugh 分期、终末期肝病评分模型或氨的影响。风险评分≥ 0.88 的亚组表现出更高比例的明显 HE(训练数据集:13.3% 与 97.4%,p < 0.001;验证数据集:0.0% 与 87.5%,p < 0.001)。
结论
我们的组合模型可以成功预测 TIPS 后明显 HE 的风险。对于低危亚组,可以安全地进行TIPS;然而,对于高危亚组,应更仔细地考虑。

























 京公网安备 11010802027423号
京公网安备 11010802027423号