JACC: Heart Failure ( IF 13.0 ) Pub Date : 2020-07-08 , DOI: 10.1016/j.jchf.2020.06.003 Thomas M Gorter 1 , Gijs van Woerden 1 , Michiel Rienstra 1 , Michael G Dickinson 1 , Yoran M Hummel 1 , Adriaan A Voors 1 , Elke S Hoendermis 1 , Dirk J van Veldhuisen 1
|
Objectives
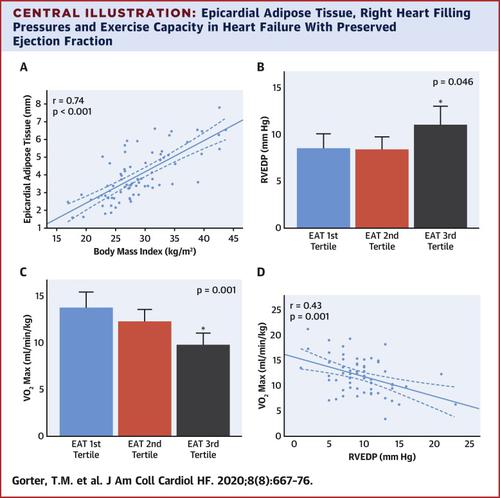
This study examined associations between epicardial adipose tissue (EAT), invasive hemodynamics, and exercise capacity in patients with heart failure with preserved ejection fraction (HFpEF).
Background
EAT is increased in patients with HFpEF and may play a role in the pathophysiology of this disorder.
Methods
Patients with heart failure and a left ventricular ejection fraction >45% who underwent right and left heart catheterization with simultaneous echocardiography were included. Pulmonary capillary wedge pressure (PCWP), left ventricular end-diastolic pressure (LVEDP), right ventricular end-diastolic pressure (RVEDP), and pulmonary vascular resistance (PVR) were invasively measured. Obesity was defined as body mass index (BMI) ≥30 kg/m2. EAT thickness alongside the right ventricle was measured on echocardiographic long- and short-axis views. Cardiopulmonary exercise testing was performed to obtain maximal oxygen uptake (VO2-max).
Results
This study examined 75 patients, mean age 74 ± 9 years; 68% were women, mean BMI was 29 ± 6 kg/m2, and 36% were obese. Higher BMI was strongly associated with increased EAT (r = 0.74; p < 0.001). Increased EAT was associated with higher RVEDP, independent of PVR (odds ratio [OR]: 1.16; 95% confidence interval [CI]: 1.02 to 1.34; p = 0.03), but not independent of obesity (p = 0.10). Increased EAT and higher RVEDP were both associated with lower VO2-max (r = −0.43; p < 0.001 and r = −0.43; p = 0.001, respectively). Increased EAT remained associated with lower VO2-max after adjustment for PVR (OR: 0.64; 95% CI: 0.49 to 0.84; p = 0.002) and obesity (OR: 0.69; 95% CI: 0.53 to 0.92; p = 0.01). EAT thickness was not associated with left-sided filling pressures (i.e., PCWP and LVEDP).
Conclusions
In HFpEF, obesity and increased EAT were associated with higher right-sided filling pressures and with reduced exercise capacity.
中文翻译:
心力衰竭的心外膜脂肪组织和有创血流动力学与保留射血分数。
目标
这项研究检查了心力衰竭患者射血分数保留(HFpEF)的心外膜脂肪组织(EAT),侵入性血流动力学和运动能力之间的关联。
背景
HFpEF患者的饮食增加,并且可能在这种疾病的病理生理中起作用。
方法
包括心力衰竭和左心室射血分数> 45%的患者,他们在同时进行超声心动图的同时进行了左右心脏导管插入术。侵入性地测量了肺毛细血管楔压(PCWP),左心室舒张末期压力(LVEDP),右心室舒张末期压力(RVEDP)和肺血管阻力(PVR)。肥胖定义为体重指数(BMI)≥30 kg / m 2。超声心动图长轴和短轴视图测量了右心室旁的EAT厚度。进行心肺运动测试以获得最大摄氧量(VO 2 -max)。
结果
这项研究检查了75名患者,平均年龄74±9岁;女性占68%,平均BMI为29±6 kg / m 2,肥胖占36%。较高的BMI与EAT增加密切相关(r = 0.74; p <0.001)。饮食增加与RVEDP升高相关,与PVR无关(赔率[OR]:1.16; 95%置信区间[CI]:1.02至1.34; p = 0.03),但与肥胖无关(p = 0.10)。更高的EAT和更高的RVEDP均与更低的VO 2 -max相关(r = -0.43; p <0.001和r = -0.43; p = 0.001)。饮食增加仍然与较低的VO 2有关调整PVR(OR:0.64; 95%CI:0.49至0.84; p = 0.002)和肥胖症(OR:0.69; 95%CI:0.53至0.92; p = 0.01)后的-max。EAT厚度与左侧填充压力(即PCWP和LVEDP)无关。
结论
在HFpEF中,肥胖和EAT升高与右侧充盈压升高和运动能力下降有关。

























 京公网安备 11010802027423号
京公网安备 11010802027423号