The American Journal of Cardiology ( IF 2.8 ) Pub Date : 2020-05-26 , DOI: 10.1016/j.amjcard.2020.05.025 Andrija Matetic 1 , Aditya Bharadwaj 2 , Mohamed O Mohamed 3 , Yashasvi Chugh 4 , Sanjay Chugh 5 , Margot Minissian 6 , Amit Amin 7 , Harriette Van Spall 8 , David L Fischman 9 , Michael Savage 9 , Annabelle Santos Volgman 10 , Mamas A Mamas 11
|
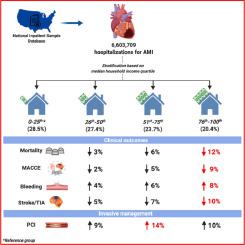
Little is known about the impact of socioeconomic status (SES) on management strategies and in-hospital clinical outcomes in patients with acute myocardial infarction (AMI) and its subtypes, and whether these trends have changed over time. All AMI hospitalizations from the National Inpatient Sample (2004 to 2014) were analyzed and stratified by zip code-based median household income (MHI) into 4 quartiles (poorest to wealthiest): 0th to 25th, 26th to 50th, 51st to 75th, and 76th to 100th. Logistic regression was performed to examine the association between MHI and AMI management strategy and in-hospital clinical outcomes. A total of 6,603,709 AMI hospitalizations were analyzed. Patients in the lowest MHI group had more co-morbidities, a worse cardiovascular risk factor profile and were more likely to be female. Differences in receipt of invasive management were observed between the lowest and highest MHI quartiles, with the lowest MHI group less likely to undergo coronary angiography (63.4% vs 64.3%, p <0.001) and percutaneous coronary intervention (40.4% vs 44.3%, p <0.001) compared with the highest MHI group, especially in the STEMI subgroup. In multivariable analysis, the highest MHI group experienced better outcomes including lower risk (adjusted odds ratio; 95% confidence intervals) of mortality (0.88; 0.88 to 0.89), MACCE (0.91; 0.91 to 0.92) and acute ischemic stroke (0.90; 0.88 to 0.91), but higher all-cause bleeding (1.08; 1.06 to 1.09) in comparison to the lowest MHI group. In conclusion, the provision of invasive management for AMI in patients with lower SES is less than patients with higher SES and is associated with worse in-hospital clinical outcomes. This work highlights the importance of ensuring equity of access and care across all strata SES.
中文翻译:
660万美国急性心肌梗死患者的社会经济状况以及管理和结果差异。
社会经济状况(SES)对急性心肌梗死(AMI)及其亚型患者的治疗策略和医院内临床结局的影响以及这些趋势是否随时间变化知之甚少。从全国住院样本(2004至2014)的所有AMI住院进行了分析,并通过拉链基于代码的家庭收入中位数(MHI)分层到4个四分位数(最穷富有):第0至25日,26日至50,51至75日,以及第76至100。进行逻辑回归分析以检查MHI和AMI管理策略与医院内临床结局之间的关联。分析了总共6,603,709例AMI住院情况。MHI最低组的患者合并症更多,心血管危险因素特征更差,女性更可能。在最低和最高的三重四分位数之间观察到侵入性管理的接受差异,最低的三重四HI组接受冠状动脉造影的可能性较小(63.4%vs 64.3%,p <0.001)和经皮冠状动脉介入治疗的可能性较小(40.4%vs 44.3%,p) <0.001)与最高MHI组相比,尤其是在STEMI亚组中。在多变量分析中,最高MHI组的病情好转,包括较低的死亡风险(调整后的优势比; 95%的置信区间)(0。88; (0.88至0.89),MACCE(0.91; 0.91至0.92)和急性缺血性卒中(0.90; 0.88至0.91),但与最低的MHI组相比,全因出血更高(1.08; 1.06至1.09)。总之,对于SES较低的患者,AMI的侵入性治疗要比SES较高的患者少,并且与院内临床预后差有关。这项工作强调了确保所有阶层SES的访问和护理公平的重要性。


























 京公网安备 11010802027423号
京公网安备 11010802027423号