Clinical Genetics ( IF 3.5 ) Pub Date : 2020-04-29 , DOI: 10.1111/cge.13753 Michele Pinelli 1, 2 , Gaetano Terrone 1 , Flavia Troglio 3 , Gabriella Maria Squeo 4 , Gerarda Cappuccio 1, 2 , Floriana Imperati 1 , Piero Pignataro 5 , Rita Genesio 5 , Lucio Nitch 5 , Ennio Del Giudice 1 , Giuseppe Merla 4 , Giuseppe Testa 3, 6, 7 , Nicola Brunetti-Pierri 1, 2
|
Recurrent deletions and duplications of 7q11.23 region are responsible for Williams‐Beuren Syndrome (WBS) and 7q11.23 microduplication syndrome (Dup7), respectively.1 Both 7q11.23 deletions and duplications typically are 1.5 Mb in size and have recurrent breakpoints. However, atypical copy number variants (CNVs) of different sizes and breakpoints affecting the 7q11.23 region have also been reported.2 Detailed phenotyping of these atypical cases can inform on the role of genes in the critical region.2 For WBS, data from both patients and animal models suggest that GTF2I is responsible for the neurodevelopmental phenotype. In contrast, the role of GTF2I in the Dup7 is less clear. To date, only one subject presenting with autism spectrum disorder without cognitive impairment and carrying an atypical duplication sparing GTF2I has been reported.3
We describe an 11‐year‐old male Caucasian proband, first child of non‐consanguineous parents with uneventful medical history until expressive language delay and learning difficulties were noted at 3 and 6 years of age, respectively. No abnormalities were detected by electroencephalography, and ophthalmologic and audiologic evaluations. Brain magnetic resonance imaging showed non‐specific gliosis in the bilateral frontal white matter and a partial empty sella without evidence of endocrine dysfunctions. Abdominal ultrasonography showed hepatomegaly with mild steatosis. At 11 years of age, his weight was 76 kg (>95th centile, z‐score = +3.2) and height 144 cm (54th centile) with a body mass index of 36.6 kg/m2 (>95th centile, z‐score = +4.6). His head circumference was 56.2 cm (81st centile). Facial features included broad forehead, straight eyebrows, narrow eyelid fissures, deep set eyes, and thin upper lip (Figure 1A). Cognitive impairment and learning difficulties were also present in his younger brother and his mother (Figure 1B). Furthermore, his maternal grandmother had gait imbalance and chronic kidney failure. Both proband's mother and grandmother attended basic school grades and occasionally worked as housekeepers. His younger sister, father and maternal grandfather had no neuro‐developmental problems by report. All three siblings were obese.

Evaluation of cognitive functioning by Wechsler Intelligence Scale for Children IV (WISC‐IV) or Wechsler Adult Intelligence Scale‐Revised (WAIS‐R) in the proband, his siblings and his mother revealed a mild cognitive impairment with homogenous involvement of functional domains in his brother and mother (Full‐scale IQ of 61, 57, 91 and 62 for the proband, his brother, his sister, and his mother, respectively). In the proband, Vineland Adaptive Behaviour Scales (VABS) showed impaired adaptive behaviour consistent with his overall intellectual functioning and no evidences of psychopathological anomalies at clinical visit or at Child Behaviour Checklist (CBCL 6‐18) testing. Maternal grandmother was unavailable for clinical and neuropsychological evaluations.
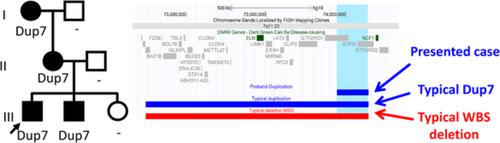
After obtaining informed consent, blood samples were collected from the proband, both his siblings, his parents and his maternal grandparents and high‐resolution array‐CGH (PerkinElmer CGX) and genomic real‐time quantitative polymerase chain reaction analyses were performed. A 7q11.23 duplication was detected in the proband, his brother, his mother and his grandmother with a minimum duplicated region spanning between nucleotides 73 944 168 and 74 138 459 (maximum interval between 73 929 917 and 74 264 323) (hg19) that partially overlapped with the typical recurrent Dup7 critical region (Figure 1B,C). The duplication was classified as variant of uncertain significance according to the consensus recommendation of the American College of Medical Genetics and Genomics (ACMG) and the Clinical Genome Resource (ClinGen)4 and included the 3′ of GTF2IRD1, the intergenic region upstream GTF2I and a portion of the 5′ of GTF2I (Figure 1D). The telomeric portion of GTF2I is embedded into two segmental duplications and thus, the telomeric breakpoint of the duplication could not be precisely determined but it appeared to overlap with the typical Dup7 telomeric breakpoint5 and involvement of NCF1 and GTF2IRD2 cannot be ruled out.
GTF2I expression was found to be elevated in peripheral blood mononuclear cells of the proband compared to controls, consistent with data previously reported in subjects with typical Dup7 (Figure 1E). Consistent with typical Dup7 phenotype,1, 5 the individuals herein presented also showed mild cognitive impairment with homogenous involvement of functional domains. In conclusion, the familial cases herein reported were found to carry a small 7q11.23 duplication that supports the role of GTF2I as critical gene for the cognitive impairment of Dup7.
中文翻译:
在具有智力障碍的家庭中进行的涉及GTF2I的小型7q11.23微复制。
7q11.23区域的重复删除和重复分别负责Williams-Beuren综合征(WBS)和7q11.23微复制综合征(Dup7)。1 7q11.23删除和重复的大小通常均为1.5 Mb,并具有经常性的断点。但是,也已经报道了影响7q11.23区域的不同大小和断点的非典型拷贝数变体(CNV)。2这些非典型病例的详细表型可以说明基因在关键区域的作用。2对于WBS,来自患者和动物模型的数据均表明GTF2I负责神经发育表型。相反,GTF2I的作用在Dup7中不太清楚。迄今为止,仅报道了一名患有自闭症谱系障碍而无认知障碍且携带非典型重复且保留GTF2I的受试者。3
我们描述了一个11岁的男性高加索先证者,他们是非血缘父母的第一个孩子,病史都很平稳,直到分别在3岁和6岁时表现出语言延迟和学习困难。脑电图,眼科和听力学评估均未发现异常。脑磁共振成像显示双侧额叶白质非特异性神经胶质增生和部分空蝶鞍,无内分泌功能障碍的证据。腹部超声检查显示肝肿大伴轻度脂肪变性。11岁那年,他的体重为76千克(> 95%,z分数= +3.2),身高144厘米(54%),体重指数为36.6 kg / m 2(> 95分,z分数= +4.6)。他的头围为56.2厘米(第81个百分位)。面部特征包括额头宽大,眉毛笔直,眼睑狭窄裂痕,深set的眼睛和薄的上唇(图1A)。他的弟弟和母亲也存在认知障碍和学习困难(图1B)。此外,他的祖母有步态不平衡和慢性肾功能衰竭。先证者的母亲和祖母都上过小学,并偶尔担任管家。据报道,他的妹妹,父亲和外祖父没有神经发育问题。三个兄弟姐妹都肥胖。
先证者,其兄弟姐妹和母亲的韦氏儿童智力量表(WISC‐IV)或韦氏成人智力量表修订版(WAIS‐R)对认知功能的评估显示出轻度认知障碍,其功能域同质参与兄弟和母亲(先证者,他的兄弟,他的妹妹和他的母亲的全面智商分别为61、57、91和62)。在先证者中,Vineland适应行为量表(VABS)显示出与他的整体智力功能相符的适应行为受损,并且在临床就诊或儿童行为清单(CBCL 6-18)测试中没有精神病理异常的证据。无法使用外婆进行临床和神经心理学评估。
在获得知情同意后,从先证者,其兄弟姐妹,其父母和其祖父母,以及高分辨率阵列CGH(PerkinElmer CGX)中收集血液样本,并进行基因组实时定量聚合酶链反应分析。在先证者,他的兄弟,他的母亲和他的祖母中检测到7q11.23重复,其最小重复区域介于核苷酸73 944 168和74 138 459之间(最大间隔为73 929 917和74 264 323之间)(hg19),与典型的复发性Dup7临界区部分重叠(图1B,C)。重复根据医学遗传学和基因组学的美国大学(ACMG)和临床基因组资源(ClinGen)的协商一致的建议列为不确定意义变异4包括GTF2IRD1的3',GTF2I上游的基因间区域和GTF2I的5'的一部分(图1D)。GTF2I的端粒部分被嵌入到两个片段重复中,因此,无法精确确定重复的端粒断裂点,但它似乎与典型的Dup7端粒断裂点5重叠,并且不能排除NCF1和GTF2IRD2的参与。
与对照组相比,先证者外周血单核细胞中的GTF2I表达升高,这与先前在典型Dup7受试者中报道的数据一致(图1E)。与典型Dup7表型,一致1,5个体本文中所呈现也表现出轻度认知损伤与功能结构域的均匀参与。总之,发现本文报道的家族病例携带7q11.23小重复片段,支持GTF2I作为Dup7认知障碍的关键基因的作用。

























 京公网安备 11010802027423号
京公网安备 11010802027423号