当前位置:
X-MOL 学术
›
JAMA Pediatr.
›
论文详情
Our official English website, www.x-mol.net, welcomes your feedback! (Note: you will need to create a separate account there.)
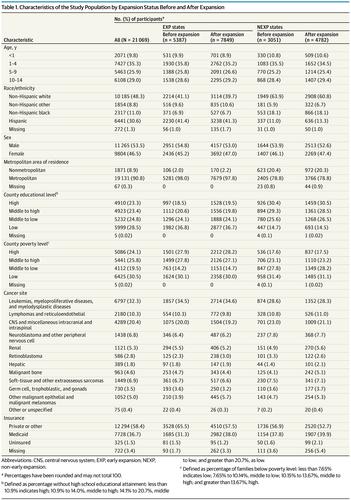
Association of Medicaid Expansion With Insurance Coverage Among Children With Cancer
JAMA Pediatrics ( IF 26.1 ) Pub Date : 2020-06-01 , DOI: 10.1001/jamapediatrics.2020.0052 Justin M Barnes 1 , Abigail R Barker 2, 3 , Allison A King 4, 5, 6, 7 , Kimberly J Johnson 2, 7
JAMA Pediatrics ( IF 26.1 ) Pub Date : 2020-06-01 , DOI: 10.1001/jamapediatrics.2020.0052 Justin M Barnes 1 , Abigail R Barker 2, 3 , Allison A King 4, 5, 6, 7 , Kimberly J Johnson 2, 7
Affiliation
|
Importance
Despite evidence of improved insurance coverage under the Affordable Care Act and Medicaid expansion among adults with cancer, little is known regarding the association of these policies with coverage among children with cancer. Objective
To assess the association of early Medicaid expansion with rates of Medicaid coverage, private coverage, and no uninsurance among children with cancer. Design, Setting, and Participants
This cross-sectional study used data from the Surveillance, Epidemiology, and End Results (SEER) database from January 1, 2007, to December 31, 2015, to identify children diagnosed with cancer at ages 0 to 14 years in the United States. Data were analyzed from July 27, 2017, to October 7, 2019. Exposures
Changes in insurance status at diagnosis after early Medicaid expansion in California, Connecticut, Washington, and New Jersey (EXP states) were compared with changes in nonexpansion (NEXP) states (Arkansas, Georgia, Hawaii, Iowa, Kentucky, Louisiana, Michigan, New Mexico, and Utah). Main Outcomes and Measures
Difference-in-differences (DID) analyses were used to compare absolute changes in insurance status (uninsured, Medicaid, private/other) at diagnosis before (2007 to 2009) and after (2011 to 2015) expansion in EXP relative to NEXP states. Results
A total of 21 069 children (11 265 [53.5%] male; mean [SD] age, 6.18 [4.57] years) were included. A 5.25% increase (95% CI, 2.61%-7.89%; P < .001) in Medicaid coverage in children with cancer was observed in EXP vs NEXP states, with larger increases among children of counties with middle to high (adjusted DID estimates, 10.18%; 95% CI, 4.22%-16.14%; P = .005) and high (adjusted DID estimates, 6.13%; 95% CI, 1.10%-11.15%; P = .05) poverty levels (P = .04 for interaction). Expansion-associated reductions of children reported as uninsured (-0.73%; 95% CI, -1.49% to 0.03%; P = .06) and with private or other insurance (-4.52%; 95% CI, -7.16% to -1.88%; P < .001) were observed. For the latter, the decrease was greater for children from counties with middle to high poverty (-9.00%; 95% CI, -14.98% to -3.02%) and high poverty (-6.38%; 95% CI, -11.36% to -1.40%) (P = .04 for interaction). Conclusions and Relevance
In this study, state Medicaid expansions were associated with increased Medicaid coverage in children with cancer overall and in some subgroups primarily owing to switching from private coverage, particularly in counties with higher levels of poverty but also through reductions in the uninsured.
中文翻译:

医疗补助扩展与癌症儿童保险范围的关联
重要性 尽管有证据表明,根据《平价医疗法案》和医疗补助计划扩大了癌症患者的保险覆盖范围,但这些政策与癌症儿童的覆盖范围之间的关联知之甚少。目的 评估早期医疗补助扩展与癌症儿童的医疗补助覆盖率、私人覆盖率和无未保险率之间的关联。设计、设置和参与者 这项横断面研究使用了 2007 年 1 月 1 日至 2015 年 12 月 31 日期间来自监测、流行病学和最终结果 (SEER) 数据库的数据,以确定 0 至 14 岁诊断为癌症的儿童在美国。数据分析时间为 2017 年 7 月 27 日至 2019 年 10 月 7 日。和新泽西州(EXP 州)与非扩张(NEXP)州(阿肯色州、乔治亚州、夏威夷州、爱荷华州、肯塔基州、路易斯安那州、密歇根州、新墨西哥州和犹他州)的变化进行了比较。主要结果和措施 差异中的差异 (DID) 分析用于比较 EXP 相对扩张之前(2007 年至 2009 年)和之后(2011 年至 2015 年)诊断时保险状况(未投保、医疗补助、私人/其他)的绝对变化到 NEXP 州。结果共纳入21 069名儿童(男性11 265 [53.5%];平均[SD]年龄,6.18 [4.57]岁)。在 EXP 和 NEXP 州,癌症儿童的医疗补助覆盖率增加了 5.25%(95% CI,2.61%-7.89%;P < .001),中高县儿童的增加幅度更大(调整后的 DID 估计) , 10.18%; 95% CI, 4.22%-16.14%; P = .005) 和高(调整后的 DID 估计,6.13%; 95% CI,1.10%-11.15%;P = .05) 贫困水平(交互作用 P = .04)。扩张相关的儿童减少报告为未投保(-0.73%;95% CI,-1.49% 至 0.03%;P = .06)和私人或其他保险(-4.52%;95% CI,-7.16% 至 - 1.88%;P < .001) 被观察到。对于后者,来自中高贫困县(-9.00%;95% CI,-14.98% 至 -3.02%)和高贫困县(-6.38%;95% CI,-11.36% 至-1.40%)(交互作用 P = .04)。结论和相关性 在这项研究中,州医疗补助的扩展与癌症儿童整体和某些亚组的医疗补助覆盖范围增加有关,这主要是由于从私人覆盖转变,特别是在贫困程度较高的县,但也通过减少未参保者。04 进行交互)。扩张相关的儿童减少报告为未投保(-0.73%;95% CI,-1.49% 至 0.03%;P = .06)和私人或其他保险(-4.52%;95% CI,-7.16% 至 - 1.88%;P < .001) 被观察到。对于后者,来自中高贫困县(-9.00%;95% CI,-14.98% 至 -3.02%)和高贫困县(-6.38%;95% CI,-11.36% 至-1.40%)(交互作用 P = .04)。结论和相关性 在这项研究中,州医疗补助的扩展与癌症儿童整体和某些亚组的医疗补助覆盖范围增加有关,这主要是由于从私人覆盖转变,特别是在贫困程度较高的县,但也通过减少未参保者。04 进行交互)。扩张相关的儿童减少报告为未投保(-0.73%;95% CI,-1.49% 至 0.03%;P = .06)和私人或其他保险(-4.52%;95% CI,-7.16% 至 - 1.88%;P < .001) 被观察到。对于后者,来自中高贫困县(-9.00%;95% CI,-14.98% 至 -3.02%)和高贫困县(-6.38%;95% CI,-11.36% 至-1.40%)(交互作用 P = .04)。结论和相关性在这项研究中,州医疗补助的扩展与癌症儿童整体和某些亚组的医疗补助覆盖范围增加有关,这主要是由于从私人覆盖转变,特别是在贫困程度较高的县,但也通过减少未参保者。-1.49% 至 0.03%;P = .06)和私人或其他保险(-4.52%;95% CI,-7.16% 至 -1.88%;P < .001)。对于后者,来自中高贫困县(-9.00%;95% CI,-14.98% 至 -3.02%)和高贫困县(-6.38%;95% CI,-11.36% 至-1.40%)(交互作用 P = .04)。结论和相关性在这项研究中,州医疗补助的扩展与癌症儿童整体和某些亚组的医疗补助覆盖范围增加有关,这主要是由于从私人覆盖转变,特别是在贫困程度较高的县,但也通过减少未参保者。-1.49% 至 0.03%;P = .06)和私人或其他保险(-4.52%;95% CI,-7.16% 至 -1.88%;P < .001)。对于后者,来自中高贫困县(-9.00%;95% CI,-14.98% 至 -3.02%)和高贫困县(-6.38%;95% CI,-11.36% 至-1.40%)(交互作用 P = .04)。结论和相关性在这项研究中,州医疗补助的扩展与癌症儿童整体和某些亚组的医疗补助覆盖范围增加有关,这主要是由于从私人覆盖转变,特别是在贫困程度较高的县,但也通过减少未参保者。来自中度至高度贫困(-9.00%;95% CI,-14.98% 至 -3.02%)和高度贫困(-6.38%;95% CI,-11.36% 至 -1.40%)县的儿童下降幅度更大(对于交互,P = .04)。结论和相关性在这项研究中,州医疗补助的扩展与癌症儿童整体和某些亚组的医疗补助覆盖范围增加有关,这主要是由于从私人覆盖转变,特别是在贫困程度较高的县,但也通过减少未参保者。来自中度至高度贫困(-9.00%;95% CI,-14.98% 至 -3.02%)和高度贫困(-6.38%;95% CI,-11.36% 至 -1.40%)县的儿童下降幅度更大(对于交互,P = .04)。结论和相关性在这项研究中,州医疗补助的扩展与癌症儿童整体和某些亚组的医疗补助覆盖范围增加有关,这主要是由于从私人覆盖转变,特别是在贫困程度较高的县,但也通过减少未参保者。
更新日期:2020-06-01
中文翻译:
医疗补助扩展与癌症儿童保险范围的关联
重要性 尽管有证据表明,根据《平价医疗法案》和医疗补助计划扩大了癌症患者的保险覆盖范围,但这些政策与癌症儿童的覆盖范围之间的关联知之甚少。目的 评估早期医疗补助扩展与癌症儿童的医疗补助覆盖率、私人覆盖率和无未保险率之间的关联。设计、设置和参与者 这项横断面研究使用了 2007 年 1 月 1 日至 2015 年 12 月 31 日期间来自监测、流行病学和最终结果 (SEER) 数据库的数据,以确定 0 至 14 岁诊断为癌症的儿童在美国。数据分析时间为 2017 年 7 月 27 日至 2019 年 10 月 7 日。和新泽西州(EXP 州)与非扩张(NEXP)州(阿肯色州、乔治亚州、夏威夷州、爱荷华州、肯塔基州、路易斯安那州、密歇根州、新墨西哥州和犹他州)的变化进行了比较。主要结果和措施 差异中的差异 (DID) 分析用于比较 EXP 相对扩张之前(2007 年至 2009 年)和之后(2011 年至 2015 年)诊断时保险状况(未投保、医疗补助、私人/其他)的绝对变化到 NEXP 州。结果共纳入21 069名儿童(男性11 265 [53.5%];平均[SD]年龄,6.18 [4.57]岁)。在 EXP 和 NEXP 州,癌症儿童的医疗补助覆盖率增加了 5.25%(95% CI,2.61%-7.89%;P < .001),中高县儿童的增加幅度更大(调整后的 DID 估计) , 10.18%; 95% CI, 4.22%-16.14%; P = .005) 和高(调整后的 DID 估计,6.13%; 95% CI,1.10%-11.15%;P = .05) 贫困水平(交互作用 P = .04)。扩张相关的儿童减少报告为未投保(-0.73%;95% CI,-1.49% 至 0.03%;P = .06)和私人或其他保险(-4.52%;95% CI,-7.16% 至 - 1.88%;P < .001) 被观察到。对于后者,来自中高贫困县(-9.00%;95% CI,-14.98% 至 -3.02%)和高贫困县(-6.38%;95% CI,-11.36% 至-1.40%)(交互作用 P = .04)。结论和相关性 在这项研究中,州医疗补助的扩展与癌症儿童整体和某些亚组的医疗补助覆盖范围增加有关,这主要是由于从私人覆盖转变,特别是在贫困程度较高的县,但也通过减少未参保者。04 进行交互)。扩张相关的儿童减少报告为未投保(-0.73%;95% CI,-1.49% 至 0.03%;P = .06)和私人或其他保险(-4.52%;95% CI,-7.16% 至 - 1.88%;P < .001) 被观察到。对于后者,来自中高贫困县(-9.00%;95% CI,-14.98% 至 -3.02%)和高贫困县(-6.38%;95% CI,-11.36% 至-1.40%)(交互作用 P = .04)。结论和相关性 在这项研究中,州医疗补助的扩展与癌症儿童整体和某些亚组的医疗补助覆盖范围增加有关,这主要是由于从私人覆盖转变,特别是在贫困程度较高的县,但也通过减少未参保者。04 进行交互)。扩张相关的儿童减少报告为未投保(-0.73%;95% CI,-1.49% 至 0.03%;P = .06)和私人或其他保险(-4.52%;95% CI,-7.16% 至 - 1.88%;P < .001) 被观察到。对于后者,来自中高贫困县(-9.00%;95% CI,-14.98% 至 -3.02%)和高贫困县(-6.38%;95% CI,-11.36% 至-1.40%)(交互作用 P = .04)。结论和相关性在这项研究中,州医疗补助的扩展与癌症儿童整体和某些亚组的医疗补助覆盖范围增加有关,这主要是由于从私人覆盖转变,特别是在贫困程度较高的县,但也通过减少未参保者。-1.49% 至 0.03%;P = .06)和私人或其他保险(-4.52%;95% CI,-7.16% 至 -1.88%;P < .001)。对于后者,来自中高贫困县(-9.00%;95% CI,-14.98% 至 -3.02%)和高贫困县(-6.38%;95% CI,-11.36% 至-1.40%)(交互作用 P = .04)。结论和相关性在这项研究中,州医疗补助的扩展与癌症儿童整体和某些亚组的医疗补助覆盖范围增加有关,这主要是由于从私人覆盖转变,特别是在贫困程度较高的县,但也通过减少未参保者。-1.49% 至 0.03%;P = .06)和私人或其他保险(-4.52%;95% CI,-7.16% 至 -1.88%;P < .001)。对于后者,来自中高贫困县(-9.00%;95% CI,-14.98% 至 -3.02%)和高贫困县(-6.38%;95% CI,-11.36% 至-1.40%)(交互作用 P = .04)。结论和相关性在这项研究中,州医疗补助的扩展与癌症儿童整体和某些亚组的医疗补助覆盖范围增加有关,这主要是由于从私人覆盖转变,特别是在贫困程度较高的县,但也通过减少未参保者。来自中度至高度贫困(-9.00%;95% CI,-14.98% 至 -3.02%)和高度贫困(-6.38%;95% CI,-11.36% 至 -1.40%)县的儿童下降幅度更大(对于交互,P = .04)。结论和相关性在这项研究中,州医疗补助的扩展与癌症儿童整体和某些亚组的医疗补助覆盖范围增加有关,这主要是由于从私人覆盖转变,特别是在贫困程度较高的县,但也通过减少未参保者。来自中度至高度贫困(-9.00%;95% CI,-14.98% 至 -3.02%)和高度贫困(-6.38%;95% CI,-11.36% 至 -1.40%)县的儿童下降幅度更大(对于交互,P = .04)。结论和相关性在这项研究中,州医疗补助的扩展与癌症儿童整体和某些亚组的医疗补助覆盖范围增加有关,这主要是由于从私人覆盖转变,特别是在贫困程度较高的县,但也通过减少未参保者。

























 京公网安备 11010802027423号
京公网安备 11010802027423号