JAMA Surgery ( IF 16.9 ) Pub Date : 2020-05-01 , DOI: 10.1001/jamasurg.2019.6384 Andrew J Meltzer 1 , M Susan Hallbeck 2, 3, 4 , Melissa M Morrow 2, 3 , Bethany R Lowndes 2, 3, 5 , Victor J Davila 1 , William M Stone 1 , Samuel R Money 1
|
The health care workforce faces numerous occupational hazards, leading to rates of injury and absenteeism that exceed those of the construction and manufacturing sectors.1,2 To date, efforts to address these problems have focused on improving safety for support staff, nurses, and allied health care personnel. Work-associated pain among surgeons has garnered less attention, despite the implications of practitioner injury and disability on the surgical workforce.3
Ergonomists have long recognized the potential hazards facing the surgeon; from the ergonomic standpoint, surgery has been described as “a mess.”4(p1011) However, research has suffered from the absence of an objective means to measure surgeons’ ergonomic stress. This study describes the ergonomic risks of surgery using wearable sensor inertial measurement units (IMUs) to monitor the ergonomics of surgeons at work and identifies risk factors for injury.
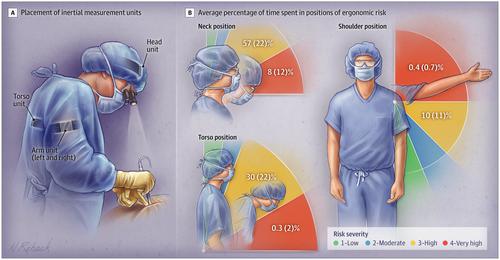
Preoperatively, surgeons had 4 IMUs placed on their head, torso, and upper arms to measure deviations from neutral body position. The IMU sensors measure body-posture angles via the fusion of data from an accelerometer, magnetometer, and gyroscope contained within each sensor. After processing, ergonomic risk was assessed by calculating the percentage of time spent in a specified range of risk categories for each body segment, facilitating stratification into ergonomic risk categories (Figure) using a validated scale.5,6 The high-risk classification was based on occupational ergonomic research exposure-response analyses, which have shown clinically significant musculoskeletal disorders and/or discomfort associated with exposure to neck, torso, and arm postures in the high-risk categories. Objectively measured ergonomic risk was compared across procedure categories (eg, open, laparoscopic, and endovascular surgeries), adjunctive equipment (eg, loupes, headlight, lead apron), as well as surgeon characteristics (eg, including self-reported case complexity and physical discomfort using a preprocedure and postprocedure survey instrument). This study was approved by the Mayo Clinic institutional review board, and oral consent was obtained from all participants. The α level was set at 5%. Statistical analyses were performed using SPSS, version 26 (IBM), and statistical significance was set at a 2-tailed P < .05.
中文翻译:
通过使用可穿戴技术来测量手术医生的人体工程学风险。
医护人员面临许多职业危害,导致的伤害和旷工率超过建筑和制造业。1 ,2迄今为止,努力解决这些问题都集中在提高安全性的技术支持人员,护士和专职卫生保健人员。尽管从业者受伤和残疾对外科手术人员有影响,但外科医生中与工作相关的疼痛引起的关注较少。3
人机工程学专家早已认识到外科医生面临的潜在危险;从人体工程学的角度来看,外科手术被描述为“一团糟”。4 (p1011)然而,由于缺乏客观的方法来测量外科医生的人体工程学压力,研究受到了困扰。这项研究描述了使用可穿戴式传感器惯性测量单元(IMU)监视手术中外科医生的人机工程学并确定受伤风险因素的人机工程学风险。
术前,外科医生在其头部,躯干和上臂放置了4个IMU,以测量与中立身体位置的偏差。IMU传感器通过融合来自每个传感器中的加速度计,磁力计和陀螺仪的数据来测量体位角。加工后,通过计算每个机体段在特定风险类别范围内花费的时间百分比,评估人机工程学风险,从而使用经过验证的量表将其分层到人体工程学风险类别中(图)。5 ,6高风险分类基于职业人体工程学研究的暴露-反应分析,该研究表明,在高风险类别中,与暴露于颈部,躯干和手臂姿势相关的临床上显着的肌肉骨骼疾病和/或不适。在各种手术类别(例如,开放式,腹腔镜和腔内手术),辅助设备(例如,放大镜,前灯,铅皮围裙)以及外科医生的特征(例如,包括自我报告的病例复杂性和物理性)之间比较了客观测量的人体工程学风险使用手术前和手术后检查工具感到不适)。这项研究已获得Mayo诊所机构审查委员会的批准,并获得了所有参与者的口头同意。α水平设定为5%。使用SPSS 26版(IBM)进行统计分析,P <.05。

























 京公网安备 11010802027423号
京公网安备 11010802027423号