PLOS Medicine ( IF 15.8 ) Pub Date : 2020-03-10 , DOI: 10.1371/journal.pmed.1003044 Tafireyi Marukutira 1, 2 , Richard T Gray 3 , Caitlin Douglass 1, 4 , Carol El-Hayek 1 , Clarissa Moreira 1 , Jason Asselin 1 , Basil Donovan 3, 5 , Tobias Vickers 3 , Tim Spelman 1 , Suzanne Crowe 1, 6 , Rebecca Guy 3 , Mark Stoove 1, 2 , Margaret Hellard 1, 2
|
Background
Globally, few studies compare progress toward the Joint United Nations Program on HIV/AIDS (UNAIDS) Fast-Track targets among migrant populations. Fast-Track targets are aligned to the HIV diagnosis and care cascade and entail achieving 90-90-90 (90% of people living with HIV [PLHIV] diagnosed, 90% of those diagnosed on treatment, and 90% of those on treatment with viral suppression [VS]) by 2020 and 95-95-95 by 2030. We compared cascades between migrant and nonmigrant populations in Australia.
Methods and findings
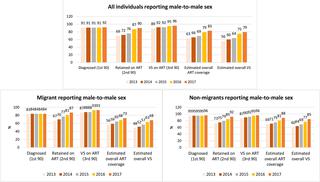
We conducted a serial cross-sectional survey for HIV diagnosis and care cascades using modelling estimates for proportions diagnosed combined with a clinical database for proportions on treatment and VS between 2013–2017. We estimated the number of PLHIV and number diagnosed using New South Wales (NSW) and Victorian (VIC) data from the Australian National HIV Registry. Cascades were stratified by migration status, sex, HIV exposure, and eligibility for subsidised healthcare in Australia (reciprocal healthcare agreement [RHCA]). We found that in 2017, 17,760 PLHIV were estimated in NSW and VIC, and 90% of them were males. In total, 90% of estimated PLHIV were diagnosed. Of the 9,391 who were diagnosed and retained in care, most (85%; n = 8,015) were males. We excluded 38% of PLHIV with missing data for country of birth, and 41% (n = 2,408) of eligible retained PLHIV were migrants. Most migrants were from Southeast Asia (SEA; 28%), northern Europe (12%), and eastern Asia (11%). Most of the migrants and nonmigrants were males (72% and 83%, respectively). We found that among those retained in care, 90% were on antiretroviral therapy (ART), and 95% of those on ART had VS (i.e., 90-90-95). Migrants had larger gaps in their HIV diagnosis and care cascade (85-85-93) compared with nonmigrants (94-90-96). Similarly, there were larger gaps among migrants reporting male-to-male HIV exposure (84-83-93) compared with nonmigrants reporting male-to-male HIV exposure (96-92-96). Large gaps were also found among migrants from SEA (72-87-93) and sub-Saharan Africa (SSA; 89-93-91). Migrants from countries ineligible for RHCA had lower cascade estimates (83-85-92) than RHCA-eligible migrants (96-86-95). Trends in the HIV diagnosis and care cascades improved over time (2013 and 2017). However, there was no significant increase in ART coverage among migrant females (incidence rate ratio [IRR]: 1.03; 95% CI 0.99–1.08; p = 0.154), nonmigrant females (IRR: 1.01; 95% CI 0.95–1.07; p = 0.71), and migrants from SEA (IRR: 1.03; 95% CI 0.99–1.07; p = 0.06) and SSA (IRR: 1.03; 95% CI 0.99–1.08; p = 0.11). Additionally, there was no significant increase in VS among migrants reporting male-to-male HIV exposure (IRR: 1.02; 95% CI 0.99–1.04; p = 0.08). The major limitation of our study was a high proportion of individuals missing data for country of birth, thereby limiting migrant status categorisation. Additionally, we used a cross-sectional instead of a longitudinal study design to develop the cascades and used the number retained as opposed to using all individuals diagnosed to calculate the proportions on ART.
Conclusions
HIV diagnosis and care cascades improved overall between 2013 and 2017 in NSW and VIC. Cascades for migrants had larger gaps compared with nonmigrants, particularly among key migrant populations. Tracking subpopulation cascades enables gaps to be identified and addressed early to facilitate achievement of Fast-Track targets.
中文翻译:
2013-2017年,澳大利亚移民的艾滋病毒诊断和关怀阶梯方面的差距:一项横断面研究。
背景
在全球范围内,很少有研究比较移民人口在实现联合国艾滋病毒/艾滋病联合规划署(UNAIDS)快速通道目标方面的进展。快速通道目标与HIV诊断和护理等级相一致,并且需要达到90-90-90(90%的诊断为HIV [PLHIV]的人,90%的接受过治疗的人和90%的接受过艾滋病毒治疗的人)病毒抑制(VS)),到2020年和2030年达到95-95-95。我们比较了澳大利亚的移民人口和非移民人口之间的级联效应。
方法和发现
我们使用2013-2017年间诊断出的比例的建模估计值与临床数据库中的治疗和VS比例进行了连续的横断面调查,用于HIV诊断和护理级联。我们根据澳大利亚国家艾滋病毒登记处的新南威尔士州(NSW)和维多利亚州(VIC)数据估算了PLHIV的数量和诊断的数量。根据移民状况,性别,艾滋病毒暴露以及在澳大利亚获得补贴医疗保健的资格(相互医疗保健协议[RHCA])对流失进行分层。我们发现,2017年在新州和维多利亚州估计有17,760例艾滋病毒感染者,其中90%是男性。总计,估计有90%的PLHIV被诊断出。在9391名被诊断并留在护理中的人中,大多数(85%;n= 8015)是男性。我们排除了38%的PLHIV患者缺少出生国的数据,而41%(n= 2,408)合格的保留的PLHIV是移民。大多数移民来自东南亚(SEA; 28%),北欧(12%)和东亚(11%)。移民和非移民大多数是男性(分别为72%和83%)。我们发现,在接受护理的患者中,有90%接受了抗逆转录病毒疗法(ART),而接受ART的患者中有95%接受了VS(即90-90-95)。与非移民(94-90-96)相比,移民在艾滋病毒的诊断和护理等级(85-85-93)方面差距更大。同样,报告男性与男性艾滋病毒接触的移民(84-83-93)与报告男性与男性艾滋病毒接触的非移民(96-92-96)相比,差距更大。在东南亚(72-87-93)和撒哈拉以南非洲地区(SSA; 89-93-91)的移民中也发现了很大的差距。不符合RHCA资格的国家的移民的级联估计数(83-85-92)比符合RHCA资格的移民(96-86-95)低。随着时间的推移,HIV诊断和护理级联的趋势有所改善(2013年和2017年)。但是,移民女性的抗逆转录病毒疗法覆盖率没有显着增加(发生率[IRR]:1.03; 95%CI 0.99–1.08;p = 0.154),非移民女性(IRR:1.01; 95%CI 0.95–1.07;p = 0.71)以及来自SEA的移民(IRR:1.03; 95%CI 0.99–1.07;p = 0.06)和SSA(IRR:1.03) ; 95%CI 0.99–1.08;p = 0.11)。此外,在报告了男性对男性艾滋病毒暴露的移民中,VS没有显着增加(IRR:1.02; 95%CI 0.99–1.04;p = 0.08)。我们研究的主要局限性是缺少出生国数据的个人比例很高,从而限制了移民身份的分类。此外,我们使用横断面而不是纵向研究设计来开发级联,并使用保留的数量,而不是使用所有诊断出的个体来计算ART的比例。
结论
在2013年至2017年之间,新南威尔士州和维多利亚州的HIV诊断和护理工作总体上有所改善。与非移民相比,移民的梯级差距更大,尤其是在主要移民人群中。跟踪亚人群的级联关系可以早日发现并解决差距,以促进实现快速跟踪目标。

























 京公网安备 11010802027423号
京公网安备 11010802027423号