当前位置:
X-MOL 学术
›
JAMA Dermatol.
›
论文详情
Our official English website, www.x-mol.net, welcomes your feedback! (Note: you will need to create a separate account there.)
Association of Race/Ethnicity and Sex With Differences in Health Care Use and Treatment for Acne.
JAMA Dermatology ( IF 10.9 ) Pub Date : 2020-02-05 , DOI: 10.1001/jamadermatol.2019.4818 John S Barbieri 1 , Daniel B Shin 1 , Shiyu Wang 1 , David J Margolis 1, 2 , Junko Takeshita 1, 2
JAMA Dermatology ( IF 10.9 ) Pub Date : 2020-02-05 , DOI: 10.1001/jamadermatol.2019.4818 John S Barbieri 1 , Daniel B Shin 1 , Shiyu Wang 1 , David J Margolis 1, 2 , Junko Takeshita 1, 2
Affiliation
|
Importance
Our understanding of potential racial/ethnic, sex, and other differences in health care use and treatment for acne is limited.
Objective
To identify potential disparities in acne care by evaluating factors associated with health care use and specific treatments for acne.
Design, Setting, and Participants
This retrospective cohort study used the Optum deidentified electronic health record data set to identify patients treated for acne from January 1, 2007, to June 30, 2017. Patients had at least 1 International Classification of Diseases, Ninth Revision (ICD-9) or International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10) code for acne and at least 1 year of continuous enrollment after the first diagnosis of acne. Data analysis was performed from September 1, 2019, to November 20, 2019.
Main Outcomes and Measures
Multivariable regression was used to quantify associations between basic patient demographic and socioeconomic characteristics and the outcomes of health care use and treatment for acne during 1 year of follow-up.
Results
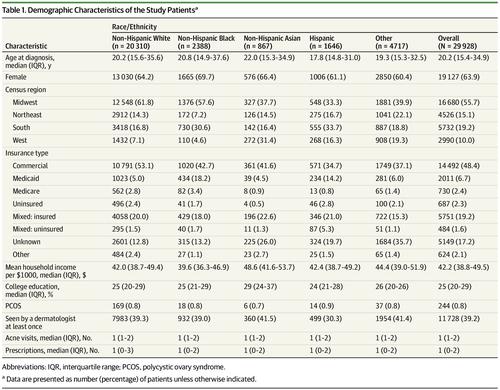
A total of 29 928 patients (median [interquartile range] age, 20.2 [15.4-34.9] years; 19 127 [63.9%] female; 20 310 [67.9%] white) met the inclusion criteria for the study. Compared with non-Hispanic white patients, non-Hispanic black patients were more likely to be seen by a dermatologist (odds ratio [OR], 1.20; 95% CI, 1.09-1.31) but received fewer prescriptions for acne medications (incidence rate ratio, 0.89; 95% CI, 0.84-0.95). Of the acne treatment options, non-Hispanic black patients were more likely to receive prescriptions for topical retinoids (OR, 1.25; 95% CI, 1.14-1.38) and topical antibiotics (OR, 1.35; 95% CI, 1.21-1.52) and less likely to receive prescriptions for oral antibiotics (OR, 0.80; 95% CI, 0.72-0.87), spironolactone (OR, 0.68; 95% CI, 0.49-0.94), and isotretinoin (OR, 0.39; 95% CI, 0.23-0.65) than non-Hispanic white patients. Male patients were more likely to be prescribed isotretinoin than female patients (OR, 2.44; 95% CI, 2.01-2.95). Compared with patients with commercial insurance, those with Medicaid were less likely to see a dermatologist (OR, 0.46; 95% CI, 0.41-0.52) or to be prescribed topical retinoids (OR, 0.82; 95% CI, 0.73-0.92), oral antibiotics (OR, 0.87; 95% CI, 0.79-0.97), spironolactone (OR, 0.50; 95% CI, 0.31-0.80), and isotretinoin (OR, 0.43; 95% CI, 0.25-0.75).
Conclusions and Relevance
The findings identify racial/ethnic, sex, and insurance-based differences in health care use and prescribing patterns for acne that are independent of other sociodemographic factors and suggest potential disparities in acne care. In particular, the study found underuse of systemic therapies among racial/ethnic minorities and isotretinoin among female patients with acne. Further study is needed to confirm and understand the reasons for these differences.
中文翻译:

种族/民族和性别与痤疮的医疗保健使用和治疗差异之间的关联。
重要性我们对潜在的种族/族裔,性别和其他在痤疮的保健使用和治疗方面的差异的理解是有限的。目的通过评估与医疗保健使用和痤疮的具体治疗有关的因素,确定痤疮护理中的潜在差异。设计,背景和参与者这项回顾性队列研究使用Optum身份不明的电子健康记录数据集来确定从2007年1月1日至2017年6月30日治疗痤疮的患者。患者至少具有1种国际疾病分类,第九版( ICD-9)或《疾病和相关健康问题国际统计分类》,第十版(ICD-10)编码痤疮,首次诊断出痤疮后至少应连续注册1年。数据分析于2019年9月1日至2019年11月20日进行。主要结果和措施在随访的1年中,使用多变量回归来量化基本患者人口统计学和社会经济特征与医疗保健和痤疮治疗结局之间的关联。结果共有29 928名患者(中位[四分位间距]年龄,20.2 [15.4-34.9]岁; 19 127 [63.9%]位女性; 20 310 [67.9%]位白人)符合纳入标准。与非西班牙裔白人患者相比,皮肤科医生更容易看到非西班牙裔黑人患者(几率[OR]为1.20; 95%CI为1.09-1.31),但痤疮药物的处方较少(发生率,0.89; 95%CI,0.84-0.95)。在痤疮治疗方案中,非西班牙裔黑人患者更有可能接受局部类维生素A的处方(OR,1.25; 95%CI,1.14-1。38)和局部抗生素(OR,1.35; 95%CI,1.21-1.52),不太可能接受口服抗生素处方(OR,0.80; 95%CI,0.72-0.87),螺内酯(OR,0.68; 95%CI) (0.49-0.94)和异维A酸(OR,0.39; 95%CI,0.23-0.65)。男性患者比女性患者更容易开异维A酸(OR,2.44; 95%CI,2.01-2.95)。与购买商业保险的患者相比,医疗补助患者看皮肤科医生的可能性较小(OR为0.46; 95%CI为0.41-0.52)或处方了局部类维生素A(OR为0.82; 95%CI为0.73-0.92),口服抗生素(OR,0.87; 95%CI,0.79-0.97),螺内酯(OR,0.50; 95%CI,0.31-0.80)和异维A酸(OR,0.43; 95%CI,0.25-0.75)。结论与相关性研究结果确定了种族/民族,性别,以及基于医疗保险的使用和痤疮处方方式的差异,这些差异与其他社会人口统计学因素无关,并暗示了痤疮护理的潜在差异。尤其是,该研究发现在种族/族裔少数人群中使用的全身疗法不足,女性痤疮患者中的异维A酸不足。需要进一步研究以确认和理解这些差异的原因。
更新日期:2020-03-12
中文翻译:
种族/民族和性别与痤疮的医疗保健使用和治疗差异之间的关联。
重要性我们对潜在的种族/族裔,性别和其他在痤疮的保健使用和治疗方面的差异的理解是有限的。目的通过评估与医疗保健使用和痤疮的具体治疗有关的因素,确定痤疮护理中的潜在差异。设计,背景和参与者这项回顾性队列研究使用Optum身份不明的电子健康记录数据集来确定从2007年1月1日至2017年6月30日治疗痤疮的患者。患者至少具有1种国际疾病分类,第九版( ICD-9)或《疾病和相关健康问题国际统计分类》,第十版(ICD-10)编码痤疮,首次诊断出痤疮后至少应连续注册1年。数据分析于2019年9月1日至2019年11月20日进行。主要结果和措施在随访的1年中,使用多变量回归来量化基本患者人口统计学和社会经济特征与医疗保健和痤疮治疗结局之间的关联。结果共有29 928名患者(中位[四分位间距]年龄,20.2 [15.4-34.9]岁; 19 127 [63.9%]位女性; 20 310 [67.9%]位白人)符合纳入标准。与非西班牙裔白人患者相比,皮肤科医生更容易看到非西班牙裔黑人患者(几率[OR]为1.20; 95%CI为1.09-1.31),但痤疮药物的处方较少(发生率,0.89; 95%CI,0.84-0.95)。在痤疮治疗方案中,非西班牙裔黑人患者更有可能接受局部类维生素A的处方(OR,1.25; 95%CI,1.14-1。38)和局部抗生素(OR,1.35; 95%CI,1.21-1.52),不太可能接受口服抗生素处方(OR,0.80; 95%CI,0.72-0.87),螺内酯(OR,0.68; 95%CI) (0.49-0.94)和异维A酸(OR,0.39; 95%CI,0.23-0.65)。男性患者比女性患者更容易开异维A酸(OR,2.44; 95%CI,2.01-2.95)。与购买商业保险的患者相比,医疗补助患者看皮肤科医生的可能性较小(OR为0.46; 95%CI为0.41-0.52)或处方了局部类维生素A(OR为0.82; 95%CI为0.73-0.92),口服抗生素(OR,0.87; 95%CI,0.79-0.97),螺内酯(OR,0.50; 95%CI,0.31-0.80)和异维A酸(OR,0.43; 95%CI,0.25-0.75)。结论与相关性研究结果确定了种族/民族,性别,以及基于医疗保险的使用和痤疮处方方式的差异,这些差异与其他社会人口统计学因素无关,并暗示了痤疮护理的潜在差异。尤其是,该研究发现在种族/族裔少数人群中使用的全身疗法不足,女性痤疮患者中的异维A酸不足。需要进一步研究以确认和理解这些差异的原因。
























 京公网安备 11010802027423号
京公网安备 11010802027423号