Bone Marrow Transplantation ( IF 4.8 ) Pub Date : 2020-02-05 , DOI: 10.1038/s41409-020-0813-9 Maria Queralt Salas 1 , Shruti Prem 1 , Eshetu G Atenafu 2 , Arjun Datt Law 1 , Wilson Lam 1 , Zeyad Al-Shaibani 1 , David Loach 1 , Dennis Dong Hwan Kim 1 , Fotios V Michelis 1 , Jeffrey Howard Lipton 1 , Rajat Kumar 1 , Jonas Mattsson 1 , Auro Viswabandya 1
|
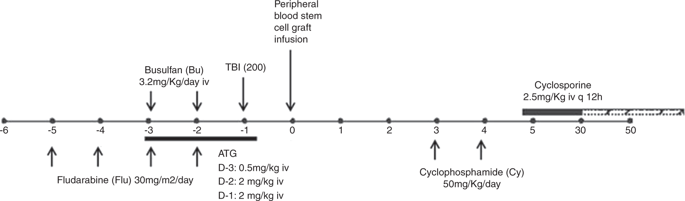
The efficacy of posttransplant cyclophosphamide (PTCy) and antithymocyte globulin (ATG) in controlling GVHD has been previously reported. We aim to study the safety and efficacy of the use of dual T-cell depletion with ATG and PTCy for peripheral blood reduced intensity conditioning regimen allo-HSCT in 270 patients with hematological malignancies. Median follow-up was 12.7 months. Nineteen percent of patients received grafts from a matched related donor, 46% from 10/10 matched unrelated donors (MUD), 16% from 9/10 MUD and 19% from haploidentical donors. Graft failure rate was 9%. CMV and EBV reactivation rates were 58 and 64%. The cumulative incidence of grade II–IV and III–IV acute GVHD at day + 100 was 20.1% and 4.6%, respectively. The CI of moderate/severe chronic GVHD at 1 year was 12.4%. There were no differences in the incidence of GVHD according to donor type. One-year OS, RFS, NRM, CIR, and GVHD-free/RFS respectively were 65.2%, 56.9%, 22.7%, 20.3%, and 47.6%. Higher disease-risk index and worse Karnofsky performance status were significant factors for poor outcomes. In conclusion, the use of T-cell dual depletion with ATG and PTCy results in very low rates of acute and chronic GVHD and acceptable relapse rates and NRM.
中文翻译:
外周血用 ATG 和 PTCy 双 T 细胞耗竭降低强度调节 allo-HSCT 导致 GVHD 发生率非常低
移植后环磷酰胺 (PTCy) 和抗胸腺细胞球蛋白 (ATG) 在控制 GVHD 方面的功效已有报道。我们的目标是研究在 270 名血液系统恶性肿瘤患者中使用 ATG 和 PTCy 双重 T 细胞耗竭对外周血降低强度预处理方案 allo-HSCT 的安全性和有效性。中位随访时间为 12.7 个月。19% 的患者接受了来自匹配相关供体的移植物,46% 来自 10/10 匹配无关供体 (MUD),16% 来自 9/10 MUD,19% 来自半相合供体。移植失败率为9%。CMV 和 EBV 再激活率分别为 58% 和 64%。在第 + 100 天,II-IV 级和 III-IV 级急性 GVHD 的累积发生率分别为 20.1% 和 4.6%。1 年时中/重度慢性 GVHD 的 CI 为 12.4%。根据供体类型,GVHD 的发生率没有差异。一年 OS、RFS、NRM、CIR 和无 GVHD/RFS 分别为 65.2%、56.9%、22.7%、20.3% 和 47.6%。较高的疾病风险指数和较差的卡诺夫斯基体能状态是不良结局的重要因素。总之,使用 ATG 和 PTCy 的 T 细胞双重耗竭导致非常低的急性和慢性 GVHD 发生率以及可接受的复发率和 NRM。


























 京公网安备 11010802027423号
京公网安备 11010802027423号