当前位置:
X-MOL 学术
›
JAMA Intern. Med.
›
论文详情
Our official English website, www.x-mol.net, welcomes your feedback! (Note: you will need to create a separate account there.)
Association of Ticagrelor vs Clopidogrel With Major Adverse Coronary Events in Patients With Acute Coronary Syndrome Undergoing Percutaneous Coronary Intervention
JAMA Internal Medicine ( IF 39.0 ) Pub Date : 2020-03-01 , DOI: 10.1001/jamainternmed.2019.6447 Ricky D Turgeon 1, 2 , Sheri L Koshman 3 , Erik Youngson 4 , Bryan Har 5 , Stephen B Wilton 5 , Matthew T James 6 , Michelle M Graham 3
JAMA Internal Medicine ( IF 39.0 ) Pub Date : 2020-03-01 , DOI: 10.1001/jamainternmed.2019.6447 Ricky D Turgeon 1, 2 , Sheri L Koshman 3 , Erik Youngson 4 , Bryan Har 5 , Stephen B Wilton 5 , Matthew T James 6 , Michelle M Graham 3
Affiliation
|
Importance
Guidelines currently recommend ticagrelor over clopidogrel for patients with acute coronary syndrome (ACS) based on randomized clinical trial data in which ticagrelor reduced major adverse coronary events (MACE) vs clopidogrel but increased bleeding and dyspnea. Objective
To compare the risk of MACE with ticagrelor vs clopidogrel in patients with ACS treated with percutaneous coronary intervention (PCI), to compare major bleeding and dyspnea, and to evaluate the association between P2Y12 inhibitor adherence and MACE. Design, Setting, and Participants
Population-based cohort study using data of patients discharged alive after PCI for ACS from the Alberta Provincial Project for Outcome Assessment in Coronary Heart Disease registry from April 1, 2012, to March 31, 2016, with follow-up to 1 year. Analysis began April 2018. Exposures
Outpatient prescription for ticagrelor or clopidogrel within 31 days after PCI. Adherence was defined as a medication refill adherence value of 80% or higher. Main Outcomes and Measures
Major adverse coronary events, a composite of all-cause death, hospitalization for ACS, unplanned coronary revascularization, or stent thrombosis within 365 days after index PCI. Secondary outcomes included hospitalization for major bleeding and emergency department visit for dyspnea. Results
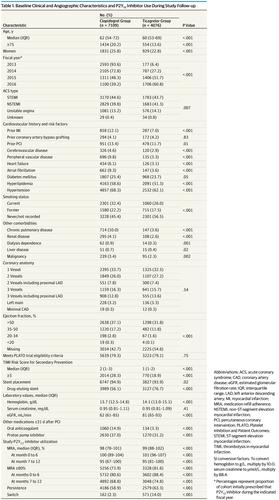
Of 11 185 individuals who underwent PCI, the median (interquartile range) age was 61 (54-71) years, and 2760 (24.7%) were women. Ticagrelor users (4076 [36.4%]) were generally younger and had fewer cardiac and noncardiac comorbidities than clopidogrel users. Ticagrelor was not associated with lower risk of MACE (adjusted hazard ratio [aHR], 0.97; 95% CI, 0.85-1.10); however, it was associated with an increased risk of major bleeding (aHR, 1.51; 95% CI, 1.29-1.78) and dyspnea (aHR, 1.98; 95% CI, 1.47-2.65). A total of 3328 ticagrelor users (81.6%) were adherent during the study vs 5256 of clopidogrel users (73.9%) (P < .001; χ2 = 86.4). In the full cohort, adherence was associated with a lower MACE risk (aHR, 0.79; 95% CI, 0.69-0.90 for adherence of ≥80% vs <80%). Differences in other secondary outcomes were not statistically significant. Sensitivity and subgroup analyses were consistent with primary analyses. Conclusions and Relevance
In this population-based cohort study of patients with ACS who underwent PCI, outpatient use of ticagrelor was not associated with a statistically significant reduction in MACE vs clopidogrel; however, it was associated with more major bleeding and dyspnea.
中文翻译:

在接受经皮冠状动脉介入治疗的急性冠状动脉综合征患者中,替格瑞洛 vs 氯吡格雷与主要不良冠状动脉事件的相关性
重要性指南目前基于随机临床试验数据推荐替格瑞洛优于氯吡格雷用于急性冠脉综合征 (ACS) 患者,其中替格瑞洛与氯吡格雷相比,可减少主要不良冠脉事件 (MACE),但会增加出血和呼吸困难。目的比较经皮冠状动脉介入治疗(PCI)治疗的ACS患者替格瑞洛与氯吡格雷发生MACE的风险,比较大出血和呼吸困难,并评估P2Y12抑制剂依从性与MACE的相关性。设计、设置和参与者 基于人群的队列研究,使用 2012 年 4 月 1 日至 2016 年 3 月 31 日阿尔伯塔省冠心病结果评估项目中 ACS 患者 PCI 后存活出院的数据,并进行随访到 1 年。分析于 2018 年 4 月开始。暴露 替格瑞洛或氯吡格雷在 PCI 后 31 天内的门诊处方。依从性被定义为 80% 或更高的药物补充依从性值。主要结果和测量指标 PCI 后 365 天内主要不良冠脉事件,包括全因死亡、ACS 住院、非计划冠脉血运重建或支架血栓形成。次要结局包括因大出血住院和因呼吸困难急诊就诊。结果 在接受 PCI 的 11 185 个人中,中位(四分位距)年龄为 61 (54-71) 岁,女性 2760 (24.7%)。与氯吡格雷使用者相比,替格瑞洛使用者 (4076 [36.4%]) 通常更年轻,心脏和非心脏合并症较少。替格瑞洛与较低的 MACE 风险无关(调整后的风险比 [aHR],0.97;95% CI,0.85-1.10);然而,它与大出血 (aHR, 1.51; 95% CI, 1.29-1.78) 和呼吸困难 (aHR, 1.98; 95% CI, 1.47-2.65) 的风险增加有关。研究期间共有 3328 名替格瑞洛使用者(81.6%)依从性,而氯吡格雷使用者为 5256 名(73.9%)(P < .001;χ2 = 86.4)。在整个队列中,依从性与较低的 MACE 风险相关(aHR,0.79;95% CI,0.69-0.90,依从性≥80% vs <80%)。其他次要结果的差异无统计学意义。敏感性和亚组分析与主要分析一致。结论和相关性 在这项针对接受 PCI 的 ACS 患者的基于人群的队列研究中,与氯吡格雷相比,替格瑞洛的门诊使用与 MACE 的统计学显着降低无关;然而,它与更多的大出血和呼吸困难有关。它与大出血 (aHR, 1.51; 95% CI, 1.29-1.78) 和呼吸困难 (aHR, 1.98; 95% CI, 1.47-2.65) 的风险增加有关。研究期间共有 3328 名替格瑞洛使用者 (81.6%) 依从性,而氯吡格雷使用者为 5256 名 (73.9%)(P < .001;χ2 = 86.4)。在整个队列中,依从性与较低的 MACE 风险相关(aHR,0.79;95% CI,0.69-0.90,依从性≥80% vs <80%)。其他次要结果的差异无统计学意义。敏感性和亚组分析与主要分析一致。结论和相关性 在这项针对接受 PCI 的 ACS 患者的基于人群的队列研究中,与氯吡格雷相比,替格瑞洛的门诊使用与 MACE 的统计学显着降低无关;然而,它与更多的大出血和呼吸困难有关。它与大出血 (aHR, 1.51; 95% CI, 1.29-1.78) 和呼吸困难 (aHR, 1.98; 95% CI, 1.47-2.65) 的风险增加有关。研究期间共有 3328 名替格瑞洛使用者 (81.6%) 依从性,而氯吡格雷使用者为 5256 名 (73.9%)(P < .001;χ2 = 86.4)。在整个队列中,依从性与较低的 MACE 风险相关(aHR,0.79;95% CI,0.69-0.90,依从性≥80% vs <80%)。其他次要结果的差异无统计学意义。敏感性和亚组分析与主要分析一致。结论和相关性 在这项针对接受 PCI 的 ACS 患者的基于人群的队列研究中,与氯吡格雷相比,替格瑞洛的门诊使用与 MACE 的统计学显着降低无关;然而,它与更多的大出血和呼吸困难有关。
更新日期:2020-03-01
中文翻译:
在接受经皮冠状动脉介入治疗的急性冠状动脉综合征患者中,替格瑞洛 vs 氯吡格雷与主要不良冠状动脉事件的相关性
重要性指南目前基于随机临床试验数据推荐替格瑞洛优于氯吡格雷用于急性冠脉综合征 (ACS) 患者,其中替格瑞洛与氯吡格雷相比,可减少主要不良冠脉事件 (MACE),但会增加出血和呼吸困难。目的比较经皮冠状动脉介入治疗(PCI)治疗的ACS患者替格瑞洛与氯吡格雷发生MACE的风险,比较大出血和呼吸困难,并评估P2Y12抑制剂依从性与MACE的相关性。设计、设置和参与者 基于人群的队列研究,使用 2012 年 4 月 1 日至 2016 年 3 月 31 日阿尔伯塔省冠心病结果评估项目中 ACS 患者 PCI 后存活出院的数据,并进行随访到 1 年。分析于 2018 年 4 月开始。暴露 替格瑞洛或氯吡格雷在 PCI 后 31 天内的门诊处方。依从性被定义为 80% 或更高的药物补充依从性值。主要结果和测量指标 PCI 后 365 天内主要不良冠脉事件,包括全因死亡、ACS 住院、非计划冠脉血运重建或支架血栓形成。次要结局包括因大出血住院和因呼吸困难急诊就诊。结果 在接受 PCI 的 11 185 个人中,中位(四分位距)年龄为 61 (54-71) 岁,女性 2760 (24.7%)。与氯吡格雷使用者相比,替格瑞洛使用者 (4076 [36.4%]) 通常更年轻,心脏和非心脏合并症较少。替格瑞洛与较低的 MACE 风险无关(调整后的风险比 [aHR],0.97;95% CI,0.85-1.10);然而,它与大出血 (aHR, 1.51; 95% CI, 1.29-1.78) 和呼吸困难 (aHR, 1.98; 95% CI, 1.47-2.65) 的风险增加有关。研究期间共有 3328 名替格瑞洛使用者(81.6%)依从性,而氯吡格雷使用者为 5256 名(73.9%)(P < .001;χ2 = 86.4)。在整个队列中,依从性与较低的 MACE 风险相关(aHR,0.79;95% CI,0.69-0.90,依从性≥80% vs <80%)。其他次要结果的差异无统计学意义。敏感性和亚组分析与主要分析一致。结论和相关性 在这项针对接受 PCI 的 ACS 患者的基于人群的队列研究中,与氯吡格雷相比,替格瑞洛的门诊使用与 MACE 的统计学显着降低无关;然而,它与更多的大出血和呼吸困难有关。它与大出血 (aHR, 1.51; 95% CI, 1.29-1.78) 和呼吸困难 (aHR, 1.98; 95% CI, 1.47-2.65) 的风险增加有关。研究期间共有 3328 名替格瑞洛使用者 (81.6%) 依从性,而氯吡格雷使用者为 5256 名 (73.9%)(P < .001;χ2 = 86.4)。在整个队列中,依从性与较低的 MACE 风险相关(aHR,0.79;95% CI,0.69-0.90,依从性≥80% vs <80%)。其他次要结果的差异无统计学意义。敏感性和亚组分析与主要分析一致。结论和相关性 在这项针对接受 PCI 的 ACS 患者的基于人群的队列研究中,与氯吡格雷相比,替格瑞洛的门诊使用与 MACE 的统计学显着降低无关;然而,它与更多的大出血和呼吸困难有关。它与大出血 (aHR, 1.51; 95% CI, 1.29-1.78) 和呼吸困难 (aHR, 1.98; 95% CI, 1.47-2.65) 的风险增加有关。研究期间共有 3328 名替格瑞洛使用者 (81.6%) 依从性,而氯吡格雷使用者为 5256 名 (73.9%)(P < .001;χ2 = 86.4)。在整个队列中,依从性与较低的 MACE 风险相关(aHR,0.79;95% CI,0.69-0.90,依从性≥80% vs <80%)。其他次要结果的差异无统计学意义。敏感性和亚组分析与主要分析一致。结论和相关性 在这项针对接受 PCI 的 ACS 患者的基于人群的队列研究中,与氯吡格雷相比,替格瑞洛的门诊使用与 MACE 的统计学显着降低无关;然而,它与更多的大出血和呼吸困难有关。


























 京公网安备 11010802027423号
京公网安备 11010802027423号