当前位置:
X-MOL 学术
›
Br. J. Surg.
›
论文详情
Our official English website, www.x-mol.net, welcomes your feedback! (Note: you will need to create a separate account there.)
Prevention of biliary fistula after partial hepatectomy by transcystic biliary drainage: randomized clinical trial.
British Journal of Surgery ( IF 9.6 ) Pub Date : 2020-01-09 , DOI: 10.1002/bjs.11405 C Maulat 1 , J-M Regimbeau 2, 3 , E Buc 4 , E Boleslawski 5 , J Belghiti 6 , J Hardwigsen 7 , E Vibert 8 , J-R Delpero 9 , E Tournay 10 , C Arnaud 10 , B Suc 1 , P Pessaux 11 , F Muscari 1
British Journal of Surgery ( IF 9.6 ) Pub Date : 2020-01-09 , DOI: 10.1002/bjs.11405 C Maulat 1 , J-M Regimbeau 2, 3 , E Buc 4 , E Boleslawski 5 , J Belghiti 6 , J Hardwigsen 7 , E Vibert 8 , J-R Delpero 9 , E Tournay 10 , C Arnaud 10 , B Suc 1 , P Pessaux 11 , F Muscari 1
Affiliation
|
BACKGROUND
Biliary fistula is one of the most common complications after hepatectomy. This study evaluated the effect of transcystic biliary drainage during hepatectomy on the occurrence of postoperative biliary fistula.
METHODS
This multicentre RCT was carried out from 2009 to 2016 in nine centres. Patients were randomized to transcystic biliary drainage or no transcystic drainage (control). Patients underwent hepatectomy (more than 2 segments) of non-cirrhotic livers. The primary endpoint was the occurrence of biliary fistula after surgery. Secondary endpoints were morbidity, postoperative mortality, duration of hospital stay, reoperation, readmission to hospital, and complications caused by catheters. Intention-to-treat and per-protocol analyses were performed.
RESULTS
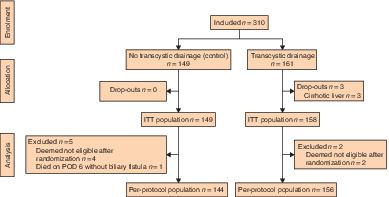
A total of 310 patients were randomized. In intention-to-treat analysis, there were 158 patients in the transcystic group and 149 in the control group. Seven patients were removed from the per-protocol analysis owing to protocol deviations. The biliary fistula rate was 5·9 per cent in intention-to-treat and 6·0 per cent in per-protocol analyses. The rate was similar in the transcystic and control groups (5·7 versus 6·0 per cent; P = 1·000). There were no differences in terms of morbidity (49·4 versus 46·3 per cent; P = 0·731), mortality (2·5 versus 4·7 per cent; P = 0·367) and reoperations (4·4 versus 10·1 per cent; P = 1·000). Median duration of hospital stay was longer in the transcystic group (11 versus 10 days; P = 0·042). The biliary fistula risk was associated with the width and length of the hepatic cut surface.
CONCLUSION
This randomized trial did not demonstrate superiority of transcystic drainage during hepatectomy in preventing biliary fistula. The use of transcystic drainage during hepatectomy to prevent postoperative biliary fistula is not recommended. Registration number: NCT01469442 ( http://www.clinicaltrials.gov).
ANTECEDENTES
La fístula biliar es una de las complicaciones más comunes después de la hepatectomía. Este estudio evalúa el efecto del drenaje biliar transcístico durante la hepatectomía en la aparición de una fístula biliar postoperatoria. MÉTODOS: Este ensayo prospectivo aleatorizado y multicéntrico (Clinical Trial NCT01469442) con dos grupos de estudio (grupo transcístico versus grupo control) se llevó a cabo de 2009 a 2016 en 9 centros. Los pacientes fueron sometidos a una hepatectomía (≥ 2 segmentos) en hígados no cirróticos. El resultado principal fue la aparición de una fístula biliar después de la cirugía. Los resultados secundarios fueron la morbilidad, la mortalidad postoperatoria, la duración de la estancia hospitalaria, la reintervención, la necesidad de reingreso y las complicaciones causadas por los catéteres. Se realizaron análisis por intención de tratamiento y por protocolo.
RESULTADOS
Un total de 310 pacientes fueron randomizados. Por intención de tratamiento, 158 pacientes fueron aleatorizados al grupo transcístico y 149 al grupo control. Siete pacientes fueron excluidos del análisis por protocolo por desviaciones del protocolo. La tasa de fístula biliar fue del 5,9% en el análisis por intención de tratamiento y del 6,0% en el análisis por protocolo. Esta tasa fue similar para el grupo transcístico y para el grupo control: 5,7% versus 6,0% (P = 1). No hubo diferencias en términos de morbilidad (49,4% versus 46,9%, P = 0,731), mortalidad (2,5% versus 4,7%, P = 0,367) y reintervenciones (4,4% versus 10,1%, P = 1). La mediana de la duración de la estancia hospitalaria fue mayor para el grupo transcístico (11 versus 10 días, P = 0,042). El riesgo de fístula biliar se correlacionó con el grosor y la longitud de la transección hepática. CONCLUSIÓN: Este ensayo aleatorizado no demuestra la superioridad del drenaje transcístico durante la hepatectomía para prevenir la fístula biliar. No se recomienda el uso de drenaje transcístico durante la hepatectomía para prevenir la fístula biliar postoperatoria.
中文翻译:

经囊性胆道引流预防部分肝切除术后胆道瘘:随机临床试验。
背景技术胆道瘘是肝切除术后最常见的并发症之一。本研究评估了肝切除术中经囊性胆道引流对术后胆道瘘管发生的影响。方法这项多中心RCT于2009年至2016年在9个中心进行。患者被随机分为经囊性胆汁引流或无经囊性引流(对照)。患者接受非肝硬化肝的肝切除术(超过2个部分)。主要终点是术后胆道瘘的发生。次要终点是发病率,术后死亡率,住院时间,再次手术,再次入院以及导管引起的并发症。进行意向治疗和按方案分析。结果共有310名患者被随机分组。在意向分析中,囊肿组158例,对照组149例。由于方案差异,从每项协议分析中删除了7名患者。意图治疗的胆道瘘率为5%·9%,按方案分析的胆道瘘率为6%·0%。在穿囊和对照组中,发生率相似(5·7%对6%·0%; P = 1·000)。在发病率(49·4比46·3%; P = 0.731),死亡率(2·5对4·7%,P = 0·367)和再次手术(4·4)方面没有差异。相对于10·1%; P = 1·000)。经囊囊组的中位住院时间较长(11天比10天; P = 0·042)。胆道瘘管的风险与肝切面的宽度和长度有关。结论该随机试验未显示肝切除术中经囊性引流在预防胆道瘘方面的优势。不建议在肝切除术中使用经囊性引流来预防术后胆瘘。注册号:NCT01469442(http://www.clinicaltrials.gov)。肝癌共同体的前身是肝癌的共同体。胆道手术后胆道切除术,胆道切除术和胆道癌切除术。墨索托斯(Métodos):预防和治疗多药(临床试验NCT01469442)在预防工作室(预防性和抗性对照)在2009年和2016年的9个百分点。Los Pacientes fueron sometidos a unahepatectomía(≥2 segmentos)enhígadosnocirróticos。埃尔·菲多拉多校长负责对cirugía的fua laapariciónde unafístulabiliardespués 事故复审单,诉讼后复活的人,医院复活的人,食品检验和复议的必要性。按照协议进行的真实性分析。结果共有310篇论文,仅供参考。由tratamiento公司负责,有158名专家进行了控制,而有149名专家进行了控制。协议分析协议书。协议中规定的5.9%的理由是不适用的。Esta tasa fue的控制效果类似,分别为5.7%和6.0%(P = 1)。无需再行静脉介入治疗(49,4%对46,9%,P = 0,731),凡尔达(2,5%对4,7%,P = 0,367)和再入院(4,4%对10,1) %,P = 1)。负责任的市长医务处处长(11对10天,P = 0,042)。埃尔·里斯戈·德·菲斯图拉·埃里克·科罗拉西奥·格罗斯·埃里·格罗斯·拉迪西克 结论:Este ensayo aleatorizado no demuestra la demerestra ladréjejetranscísticodurante lahepatectomíapara prevenir lafístulabiliar。没有人可以在胆道癌术后再进行肝切除术。负责任的市长医务处处长(11对10天,P = 0,042)。埃尔·里斯戈·德·菲斯图拉·埃里克·科罗拉西奥·埃斯·格里索(La grosor y la la longitud de latransecciónhepática)。结论:Este ensayo aleatorizado no demuestra la demerestra ladréjejetranscísticodurante lahepatectomíapara prevenir lafístulabiliar。没有胆囊切除术后胆囊切除术的建议。负责任的市长医务处处长(11对10天,P = 0,042)。埃尔·里斯戈·德·菲斯图拉·埃里克·科罗拉西奥·埃斯·格里索(La grosor y la la longitud de latransecciónhepática)。结论:Este ensayo aleatorizado no demuestra la demerestra ladréjejetranscísticodurante lahepatectomíapara prevenir lafístulabiliar。没有胆囊切除术后胆囊切除术的建议。
更新日期:2020-01-09
中文翻译:
经囊性胆道引流预防部分肝切除术后胆道瘘:随机临床试验。
背景技术胆道瘘是肝切除术后最常见的并发症之一。本研究评估了肝切除术中经囊性胆道引流对术后胆道瘘管发生的影响。方法这项多中心RCT于2009年至2016年在9个中心进行。患者被随机分为经囊性胆汁引流或无经囊性引流(对照)。患者接受非肝硬化肝的肝切除术(超过2个部分)。主要终点是术后胆道瘘的发生。次要终点是发病率,术后死亡率,住院时间,再次手术,再次入院以及导管引起的并发症。进行意向治疗和按方案分析。结果共有310名患者被随机分组。在意向分析中,囊肿组158例,对照组149例。由于方案差异,从每项协议分析中删除了7名患者。意图治疗的胆道瘘率为5%·9%,按方案分析的胆道瘘率为6%·0%。在穿囊和对照组中,发生率相似(5·7%对6%·0%; P = 1·000)。在发病率(49·4比46·3%; P = 0.731),死亡率(2·5对4·7%,P = 0·367)和再次手术(4·4)方面没有差异。相对于10·1%; P = 1·000)。经囊囊组的中位住院时间较长(11天比10天; P = 0·042)。胆道瘘管的风险与肝切面的宽度和长度有关。结论该随机试验未显示肝切除术中经囊性引流在预防胆道瘘方面的优势。不建议在肝切除术中使用经囊性引流来预防术后胆瘘。注册号:NCT01469442(http://www.clinicaltrials.gov)。肝癌共同体的前身是肝癌的共同体。胆道手术后胆道切除术,胆道切除术和胆道癌切除术。墨索托斯(Métodos):预防和治疗多药(临床试验NCT01469442)在预防工作室(预防性和抗性对照)在2009年和2016年的9个百分点。Los Pacientes fueron sometidos a unahepatectomía(≥2 segmentos)enhígadosnocirróticos。埃尔·菲多拉多校长负责对cirugía的fua laapariciónde unafístulabiliardespués 事故复审单,诉讼后复活的人,医院复活的人,食品检验和复议的必要性。按照协议进行的真实性分析。结果共有310篇论文,仅供参考。由tratamiento公司负责,有158名专家进行了控制,而有149名专家进行了控制。协议分析协议书。协议中规定的5.9%的理由是不适用的。Esta tasa fue的控制效果类似,分别为5.7%和6.0%(P = 1)。无需再行静脉介入治疗(49,4%对46,9%,P = 0,731),凡尔达(2,5%对4,7%,P = 0,367)和再入院(4,4%对10,1) %,P = 1)。负责任的市长医务处处长(11对10天,P = 0,042)。埃尔·里斯戈·德·菲斯图拉·埃里克·科罗拉西奥·格罗斯·埃里·格罗斯·拉迪西克 结论:Este ensayo aleatorizado no demuestra la demerestra ladréjejetranscísticodurante lahepatectomíapara prevenir lafístulabiliar。没有人可以在胆道癌术后再进行肝切除术。负责任的市长医务处处长(11对10天,P = 0,042)。埃尔·里斯戈·德·菲斯图拉·埃里克·科罗拉西奥·埃斯·格里索(La grosor y la la longitud de latransecciónhepática)。结论:Este ensayo aleatorizado no demuestra la demerestra ladréjejetranscísticodurante lahepatectomíapara prevenir lafístulabiliar。没有胆囊切除术后胆囊切除术的建议。负责任的市长医务处处长(11对10天,P = 0,042)。埃尔·里斯戈·德·菲斯图拉·埃里克·科罗拉西奥·埃斯·格里索(La grosor y la la longitud de latransecciónhepática)。结论:Este ensayo aleatorizado no demuestra la demerestra ladréjejetranscísticodurante lahepatectomíapara prevenir lafístulabiliar。没有胆囊切除术后胆囊切除术的建议。


























 京公网安备 11010802027423号
京公网安备 11010802027423号