Our official English website, www.x-mol.net, welcomes your feedback! (Note: you will need to create a separate account there.)
Effectiveness of a scalable group-based education and monitoring program, delivered by health workers, to improve control of hypertension in rural India: A cluster randomised controlled trial.
PLOS Medicine ( IF 15.8 ) Pub Date : 2020-01-02 , DOI: 10.1371/journal.pmed.1002997 Dilan Giguruwa Gamage 1 , Michaela A Riddell 1 , Rohina Joshi 2, 3, 4 , Kavumpurathu R Thankappan 5 , Clara K Chow 2, 3, 6 , Brian Oldenburg 7 , Roger G Evans 8 , Ajay S Mahal 9, 10 , Kartik Kalyanram 11 , Kamakshi Kartik 11 , Oduru Suresh 1, 11 , Nihal Thomas 12 , Gomathyamma K Mini 5, 13 , Pallab K Maulik 2, 4, 14 , Velandai K Srikanth 1, 15 , Simin Arabshahi 1 , Ravi P Varma 5 , Rama K Guggilla 4, 16 , Fabrizio D'Esposito 7 , Thirunavukkarasu Sathish 7, 17 , Mohammed Alim 4, 18 , Amanda G Thrift 1
PLOS Medicine ( IF 15.8 ) Pub Date : 2020-01-02 , DOI: 10.1371/journal.pmed.1002997 Dilan Giguruwa Gamage 1 , Michaela A Riddell 1 , Rohina Joshi 2, 3, 4 , Kavumpurathu R Thankappan 5 , Clara K Chow 2, 3, 6 , Brian Oldenburg 7 , Roger G Evans 8 , Ajay S Mahal 9, 10 , Kartik Kalyanram 11 , Kamakshi Kartik 11 , Oduru Suresh 1, 11 , Nihal Thomas 12 , Gomathyamma K Mini 5, 13 , Pallab K Maulik 2, 4, 14 , Velandai K Srikanth 1, 15 , Simin Arabshahi 1 , Ravi P Varma 5 , Rama K Guggilla 4, 16 , Fabrizio D'Esposito 7 , Thirunavukkarasu Sathish 7, 17 , Mohammed Alim 4, 18 , Amanda G Thrift 1
Affiliation
|
BACKGROUND
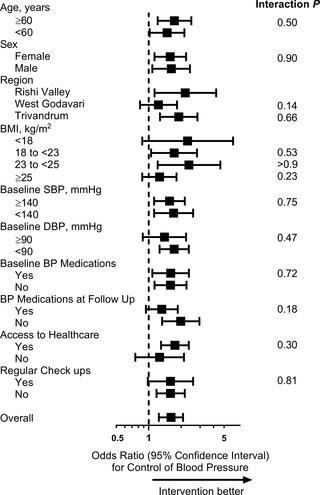
New methods are required to manage hypertension in resource-poor settings. We hypothesised that a community health worker (CHW)-led group-based education and monitoring intervention would improve control of blood pressure (BP).
METHODS AND FINDINGS
We conducted a baseline community-based survey followed by a cluster randomised controlled trial of people with hypertension in 3 rural regions of South India, each at differing stages of epidemiological transition. Participants with hypertension, defined as BP ≥ 140/90 mm Hg or taking antihypertensive medication, were advised to visit a doctor. In each region, villages were randomly assigned to intervention or usual care (UC) in a 1:2 ratio. In intervention clusters, trained CHWs delivered a group-based intervention to people with hypertension. The program, conducted fortnightly for 3 months, included monitoring of BP, education about hypertension, and support for healthy lifestyle change. Outcomes were assessed approximately 2 months after completion of the intervention. The primary outcome was control of BP (BP < 140/90 mm Hg), analysed using mixed effects regression, clustered by village within region and adjusted for baseline control of hypertension (using intention-to-treat principles). Of 2,382 potentially eligible people, 637 from 5 intervention clusters and 1,097 from 10 UC clusters were recruited between November 2015 and April 2016, with follow-up occurring in 459 in the intervention group and 1,012 in UC. Mean age was 56.9 years (SD 13.7). Baseline BP was similar between groups. Control of BP improved from baseline to follow-up more in the intervention group (from 227 [49.5%] to 320 [69.7%] individuals) than in the UC group (from 528 [52.2%] to 624 [61.7%] individuals) (odds ratio [OR] 1.6, 95% CI 1.2-2.1; P = 0.001). In secondary outcome analyses, there was a greater decline in systolic BP in the intervention than UC group (-5.0 mm Hg, 95% CI -7.1 to -3.0; P < 0.001) and a greater decline in diastolic BP (-2.1 mm Hg, 95% CI -3.6 to -0.6; P < 0.006), but no detectable difference in the use of BP-lowering medications between groups (OR 1.2, 95% CI 0.8-1.9; P = 0.34). Similar results were found when using imputation analyses that included those lost to follow-up. Limitations include a relatively short follow-up period and use of outcome assessors who were not blinded to the group allocation.
CONCLUSIONS
While the durability of the effect is uncertain, this trial provides evidence that a low-cost program using CHWs to deliver an education and monitoring intervention is effective in controlling BP and is potentially scalable in resource-poor settings globally.
TRIAL REGISTRATION
The trial was registered with the Clinical Trials Registry-India (CTRI/2016/02/006678).
中文翻译:

由卫生工作者实施的可扩展的基于小组的教育和监控计划对改善印度农村地区高血压的控制的有效性:一项集群随机对照试验。
背景技术需要新的方法来在资源匮乏的环境中管理高血压。我们假设由社区卫生工作者(CHW)领导的基于小组的教育和监测干预将改善对血压(BP)的控制。方法和研究结果我们进行了一项基于社区的基线调查,随后在印度南部3个农村地区进行了一项随机分组的高血压人群随机对照试验,每个地区都处于流行病学转变的不同阶段。建议患有高血压的患者定义为BP≥140/90 mm Hg或正在服用降压药。在每个区域中,将村庄按1:2的比例随机分配给干预或常规护理(UC)。在干预小组中,训练有素的社区卫生工作者为高血压患者提供了基于小组的干预。该程序,每两周进行一次,为期3个月,包括对BP的监测,对高血压的教育以及对健康生活方式的支持。干预完成后约2个月评估结果。主要结果是控制血压(BP <140/90 mm Hg),使用混合效应回归分析,按区域内的村庄进行聚类,并针对高血压的基线控制进行了调整(使用意向性治疗原则)。在2015年11月至2016年4月之间,在2382名潜在合格人员中,招募了来自5个干预小组的637人和来自10个UC小组的1097人,随访了干预组的459人和UC的1012人。平均年龄为56.9岁(SD 13.7)。两组之间的基线血压相似。血压控制从基线水平提高到干预组的更多随访(从227起[49]。UC组(从528 [52.2%]到624 [61.7%]个个体)从5%]增至320 [69.7%])(赔率[OR] 1.6、95%CI 1.2-2.1; P = 0.001) 。在次要结局分析中,干预组的收缩压下降比UC组更大(-5.0 mm Hg,95%CI -7.1至-3.0; P <0.001),舒张压下降更大(-2.1 mm Hg) ,95%CI -3.6至-0.6; P <0.006),但两组之间使用降血压药物的差异无统计学意义(OR 1.2,95%CI 0.8-1.9; P = 0.34)。当使用归因分析(包括因随访而丢失的归因分析)时,发现了相似的结果。局限性包括相对较短的随访时间和对小组分配不知情的结果评估者的使用。结论虽然效果的持久性不确定,该试验提供的证据表明,使用CHW进行教育和监控干预的低成本计划可有效控制BP,并且在全球资源匮乏的环境中具有可扩展性。试验注册该试验已在印度临床试验注册中心(CTRI / 2016/02/006678)进行了注册。
更新日期:2020-01-04
中文翻译:
由卫生工作者实施的可扩展的基于小组的教育和监控计划对改善印度农村地区高血压的控制的有效性:一项集群随机对照试验。
背景技术需要新的方法来在资源匮乏的环境中管理高血压。我们假设由社区卫生工作者(CHW)领导的基于小组的教育和监测干预将改善对血压(BP)的控制。方法和研究结果我们进行了一项基于社区的基线调查,随后在印度南部3个农村地区进行了一项随机分组的高血压人群随机对照试验,每个地区都处于流行病学转变的不同阶段。建议患有高血压的患者定义为BP≥140/90 mm Hg或正在服用降压药。在每个区域中,将村庄按1:2的比例随机分配给干预或常规护理(UC)。在干预小组中,训练有素的社区卫生工作者为高血压患者提供了基于小组的干预。该程序,每两周进行一次,为期3个月,包括对BP的监测,对高血压的教育以及对健康生活方式的支持。干预完成后约2个月评估结果。主要结果是控制血压(BP <140/90 mm Hg),使用混合效应回归分析,按区域内的村庄进行聚类,并针对高血压的基线控制进行了调整(使用意向性治疗原则)。在2015年11月至2016年4月之间,在2382名潜在合格人员中,招募了来自5个干预小组的637人和来自10个UC小组的1097人,随访了干预组的459人和UC的1012人。平均年龄为56.9岁(SD 13.7)。两组之间的基线血压相似。血压控制从基线水平提高到干预组的更多随访(从227起[49]。UC组(从528 [52.2%]到624 [61.7%]个个体)从5%]增至320 [69.7%])(赔率[OR] 1.6、95%CI 1.2-2.1; P = 0.001) 。在次要结局分析中,干预组的收缩压下降比UC组更大(-5.0 mm Hg,95%CI -7.1至-3.0; P <0.001),舒张压下降更大(-2.1 mm Hg) ,95%CI -3.6至-0.6; P <0.006),但两组之间使用降血压药物的差异无统计学意义(OR 1.2,95%CI 0.8-1.9; P = 0.34)。当使用归因分析(包括因随访而丢失的归因分析)时,发现了相似的结果。局限性包括相对较短的随访时间和对小组分配不知情的结果评估者的使用。结论虽然效果的持久性不确定,该试验提供的证据表明,使用CHW进行教育和监控干预的低成本计划可有效控制BP,并且在全球资源匮乏的环境中具有可扩展性。试验注册该试验已在印度临床试验注册中心(CTRI / 2016/02/006678)进行了注册。

























 京公网安备 11010802027423号
京公网安备 11010802027423号