
Abstract
Background
Several studies have utilised isometric, eccentric and downhill walking pre-conditioning as a strategy for alleviating the signs and symptoms of exercise-induced muscle damage (EIMD) following a bout of damaging physical activity.
Objectives
This systematic review and meta-analysis examined the effects of pre-conditioning strategies on indices of muscle damage and physical performance measures following a second bout of strenuous physical activity.
Data Sources
PubMed, CINAHL and Scopus.
Eligibility Criteria
Studies meeting the PICO (population, intervention/exposure, comparison, and outcome) criteria were included in this review: (1) general population or “untrained” participants with no contraindications affecting physical performance; (2) studies with a parallel design to examine the prevention and severity of muscle-damaging contractions; (3) outcome measures were compared using baseline and post-intervention measures; and (4) outcome measures included any markers of indirect muscle damage and muscular contractility measures.
Participants
Individuals with no resistance training experiences in the previous 6 or more months.
Interventions
A single bout of pre-conditioning exercises consisting of eccentric or isometric contractions performed a minimum of 24 h prior to a bout of damaging physical activity were compared to control interventions that did not perform pre-conditioning prior to damaging physical activity.
Study Appraisal
Kmet appraisal system.
Synthesis Methods
Quantitative analysis was conducted using forest plots to examine standardised mean differences (SMD, i.e. effect size), test statistics for statistical significance (i.e. Z-values) and between-study heterogeneity by inspecting I2.
Results
Following abstract and full-text screening, 23 articles were included in this paper. Based on the meta-analysis, the pre-conditioning group exhibited lower levels of creatine kinase at 24 h (SMD = − 1.64; Z = 8.39; p = 0.00001), 48 h (SMD = − 2.65; Z = 7.78; p = 0.00001), 72 h (SMD = − 2.39; Z = 5.71; p = 0.00001) and 96 h post-exercise (SMD = − 3.52; Z = 7.39; p = 0.00001) than the control group. Delayed-onset muscle soreness was also lower for the pre-conditioning group at 24 h (SMD = − 1.89; Z = 6.17; p = 0.00001), 48 h (SMD = − 2.50; Z = 7.99; p = 0.00001), 72 h (SMD = − 2.73; Z = 7.86; p = 0.00001) and 96 h post-exercise (SMD = − 3.30; Z = 8.47; p = 0.00001). Maximal voluntary contraction force was maintained and returned to normal sooner in the pre-conditioning group than in the control group, 24 h (SMD = 1.46; Z = 5.49; p = 0.00001), 48 h (SMD = 1.59; Z = 6.04; p = 0.00001), 72 h (SMD = 2.02; Z = 6.09; p = 0.00001) and 96 h post-exercise (SMD = 2.16; Z = 5.69; p = 0.00001). Range of motion was better maintained by the pre-conditioning group compared with the control group at 24 h (SMD = 1.48; Z = 4.30; p = 0.00001), 48 h (SMD = 2.20; Z = 5.64; p = 0.00001), 72 h (SMD = 2.66; Z = 5.42; p = 0.00001) and 96 h post-exercise (SMD = 2.5; Z = 5.46; p = 0.00001). Based on qualitative analyses, pre-conditioning activities were more effective when performed at 2–4 days before the muscle-damaging protocol compared with immediately prior to the muscle-damaging protocol, or 1–3 weeks prior to the muscle-damaging protocol. Furthermore, pre-conditioning activities performed using eccentric contractions over isometric contractions, with higher volumes, greater intensity and more lengthened muscle contractions provided greater protection from EIMD.
Limitations
Several outcome measures showed high inter-study heterogeneity. The inability to account for differences in durations between pre-conditioning and the second bout of damaging physical activity was also limiting.
Conclusions
Pre-conditioning significantly reduced the severity of creatine kinase release, delayed-onset muscle soreness, loss of maximal voluntary contraction force and the range of motion decrease. Pre-conditioning may prevent severe EIMD and accelerate recovery of muscle force generation capacity.
Similar content being viewed by others
Exercise-induced muscle damage (EIMD) decreases the functional capacity of untrained individuals, following strenuous physical activity. |
Performing pre-conditioning activities several days to weeks prior to strenuous physical activity reduces the severity of EIMD and decreases recovery time. |
Pre-conditioning activities appear to be most effective if performed 2–4 days prior to muscle-damaging exercises, and with greater volume and intensity. |
Although greater volume and intensity of pre-conditioning activities may cause EIMD, the level of EIMD is notably lower than the initial exposure to EIMD exercises, indicating that pre-conditioning activities may be effective in reducing the level of EIMD following initial exposure to unfamiliar strenuous exercises. |
1 Introduction
Exercise-induced muscle damage (EIMD) is a phenomenon that typically occurs after a bout of intense physical exertion, with eccentric muscle contractions causing the highest degree of damage because of forced lengthening during the cross-bridge cycle [1]. Exercise-induced muscle damage normally occurs within 48 h and can last between 2 and 10 days. Symptoms include localised muscle soreness (delayed-onset muscle soreness, [DOMS]) and swelling, increased blood biomarkers caused by muscle cell damage (e.g. creatine kinase [CK]), decreased voluntary force production and an increase in the perceived difficulty of movement [2,3,4]. These symptoms result in detrimental effects during subsequent training sessions, such as reductions in force and power output, impaired proprioception and movement compensation, and decreased training effort, thus impairing the quality of training and increasing the potential for injury in athletes [5, 6].
Once EIMD occurs because of strenuous exercise, a subsequent bout of an equivalent activity will result in less severe EIMD, known as the repeated bout effect (RBE) [7,8,9]. Musculoskeletal structures exposed to a previously damaging stimulus are protected against a subsequent large EIMD response due to neural and structural adaptation, including improved motor unit recruitment and a rate of force production increase [8]. Hence, once an acute adaptation occurs, the musculoskeletal structures exhibit accelerated recovery dynamics following a strenuous bout of exercise. Various studies have observed the duration of protection against EIMD, with the level of protection being maintained for 2–8 weeks after the first bout of eccentric exercise [10,11,12], and approximately 6 months until return to conditions prior to the muscle-damaging exposure [9].
The traditional form of RBE would require greater recovery following the initial bout of exercise, given the initial exposure to high levels of physiological stress and the undesirable signs and symptoms of EIMD before undertaking subsequent training bouts. To circumvent these training difficulties, studies have attempted to attenuate EIMD using lesser damaging to non-damaging pre-conditioning activities. Several types of pre-conditioning activities have been examined, including: low-intensity and volume eccentric contractions that range from 10 to 40% of maximum contraction effort [13, 14]; short duration (3–5 s) maximal voluntary contractions (MVCs) repeated several times [10, 15] and short duration downhill walking (5 min) utilising the eccentric nature of a downhill gait to attenuate damage induced by the long duration of downhill walking a week later [16]. These pre-conditioning interventions produced no measurable change in indirect biomarkers of EIMD (e.g. CK), and did not produce DOMS, inflammation or an extended reduction in force production [17,18,19]. Furthermore, participants exposed to various pre-conditioning activities demonstrated significantly lower CK and DOMS values, whilst force production measures recovered sooner after muscle-damaging exercises, when compared with control groups. However, pre-conditioning strategies also have a short duration of effectiveness and are required to be performed 1 day to 2 weeks prior to any muscle-damaging activity, with 24–48 h as the preferred time period for isometric contractions [15, 17, 20] and weeks for non-damaging eccentric muscle contractions [21,22,23]. Whilst not fully understood, it is believed that pre-conditioning activities exhibit protection against EIMD using similar mechanisms to that of traditional RBE, such as neurological priming, extra-cellular matrix remodelling and pennation angle changes to provide a short-term adaptation, allowing greater transmission of force and improved joint congruency while maintaining neural excitation [4, 24,25,26]. More recent evidence also indicates a smaller displacement of the myotendinous junction as a potential of the pre-conditioning effect on muscle damage [27]. Therefore, the pre-conditioning effect and RBE both exhibit protection from EIMD following the subsequent muscle-damaging bouts and are underpinned by similar mechanisms. However, with the pre-conditioning effect, the exercises during the first bout are deliberately selected to lower the level of EIMD (e.g. lower intensity, lower volume, shorter muscle length) in preparation for a more intense second bout of muscle-damaging exercises. Conversely, the RBE phenomenon is usually considered when the muscle-damaging exercises are prescribed similarly, if not identically, between the first and subsequent bouts with the intention to cause a high level of EIMD following the first bout.
Given the ability to induce an RBE with minimal EIMD symptomatology, pre-conditioning activities may be a useful tool for rehabilitation or concurrent training scenarios where high levels of EIMD are expected, although are not desirable. For example, attenuating EIMD for athletes returning to resistance training after a long hiatus because of an injury may decrease the recovery time needed between rehabilitation sessions, and thereby speed up the return to play time [14]. Individuals considering introducing resistance exercises as part of their normal training programme, such as endurance athletes or youth athletes, may also consider pre-conditioning activities to minimise the level of EIMD during the initial period of a resistance training programme.
There is clear evidence to date regarding the effectiveness implementing pre-conditioning activities prior to muscle-damaging protocols to ameliorate the level of EIMD. However, the methodologies used to implement pre-conditioning thus far have varied. For example, including short- and long-duration MVC appears to have a potent prophylactic effect against EIMD when used prior to high-intensity eccentric contractions [10, 17]. Low-intensity eccentric contractions, low-volume eccentric contractions and downhill walking have been performed on various muscle groups, attenuating a second more intense bout of eccentric contractions without first causing EIMD [20, 23, 28]. Because of the variety of contraction times, intensities and volumes used for pre-conditioning all reducing EIMD with some degree of effectiveness, it is difficult for the practitioner to discern best pre-conditioning practice. A recent review examining the effect of isometric pre-conditioning highlighted that isometric pre-conditioning attenuates EIMD in populations with little or no prior eccentric contraction exposure. However, the review highlighted that pre-conditioning has not yet been explored in a trained population and may not be effective, owing to the long-term prophylactic effects of eccentric contractions [29]. This review also postulated that the potency of attenuation of EIMD may be related to the number of maximal isometric contractions. However, to date, no appraisal of the quality of studies examining isometric or EPC has been completed, nor a meta-analysis conducted based on pooled data of multiple studies. Therefore, a systematic review and meta-analysis are warranted to provide insight into the effectiveness of these different pre-conditioning strategies. Consequently, the aim of the current systematic review and meta-analysis is to evaluate the effectiveness of pre-conditioning strategies in preventing EIMD, give some insight to practitioners regarding implementation and to highlight areas of further research.
2 Methods
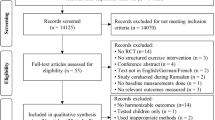
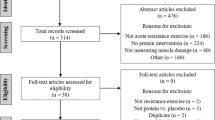
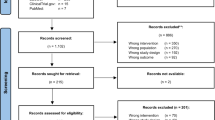
This systematic review and meta-analysis used the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines [30] for the methodology and reporting of data (Fig. 1). A PICO (population, intervention/exposure, comparison and outcome) approach was followed to determine study eligibility and inclusion in this review.

Selection process detailing the search procedure for assessing eligibility for inclusion in a systematic review and meta-analysis
2.1 Inclusion/Exclusion Criteria
Studies meeting the following PICO criteria were included in this review.
-
1.
Population healthy adults.
-
2.
Intervention studies with a parallel (between-group) design to examine the prevention and severity of muscle-damaging contractions following a bout of pre-condition exercises (e.g. a single bout of 10% pre-conditioning eccentric contractions prior to a single bout of 50 maximal eccentric contractions in the pre-conditioning group compared with a control group that performed a single bout of 50 maximal eccentric contractions without pre-conditioning activities).
-
3.
Comparison outcome measures were compared between groups based on measures at 24 h, 48 h, 72 h and 96 h after the muscle-damaging protocol.
-
4.
Outcome outcome measures included common markers of indirect muscle damage (e.g. CK, DOMS, joint range of motion [ROM]) and muscular contractility measures (e.g. isometric force and isokinetic torque).
Studies were excluded if: (1) they were reported in a language other than English with no translation; (2) they were clinical in nature (i.e. participants were recovering from a trauma such as a stroke or injury); (3) no clear measures of EIMD were reported; (4) no comparative groups were presented; and (5) they were reported as abstracts, reviews or case studies.
2.2 Search Strategy
The following literature search was performed on 7 April, 2022 across three electronic databases (PubMed, CINAHL and Scopus). For the PubMed search, mesh terms were employed with separate strings, including: (1) Humans; (2) Muscle-damage protocols (Exercise or Exercise therapy/methods or Physical conditioning, human/adverse effects or Physical conditioning, human/methods or Exercise test or Physical exertion/physiology or Resistance training/methods or Resistance training/adverse effects); and (3) muscle damage markers (Creatine kinase or Myoglobin or L-Lactate Dehydrogenase or Interleukin-6 or Interleukin-8 or Interleukin-1 or C-Reactive Protein"[Mesh] or Tumour Necrosis Factor-alpha"[Mesh] or Inflammation or Oxidative stress or Pain/etiology or Myalgia or Musculoskeletal pain and Muscle, skeletal or Quadriceps muscle or" or Arm or Elbow joint or Knee joint). A free text search was also conducted in PubMed to source papers that were currently in press, including: (Muscle Damage or Creatine Kinase or Myoglobin or Lactate Dehydrogenase or Muscle Soreness, or Interleukin 6 or Interleukin 8 or C-reactive Protein or Tumour Necrosis Factor or TNF or Oxidative Stress) and (Eccentric or Concentric or Isometric or Pre-conditioning or Priming) and (Repeated Bout or Second Bout or Subsequent Bout or Alleviat* or Recover* or Adapt* or Adaptation). An equivalent free text search was used for the Cinahl and Scopus databases. Furthermore, reference lists from included studies were screened as a supplementary search.
2.3 Selection Process
A list of abstracts extracted from the literature search was screened for eligibility by two authors with sport and exercise science backgrounds (LB and BDT). Abstracts were classified as either meeting the inclusion criteria (yes) or not meeting the inclusion criteria (no). Once screening was completed, the full texts of all included abstracts were further screened using the same inclusion criteria. Any discrepancies for the screening of the abstracts and the full-text search between the two authors involved a third author (KD), until a consensus was reached.
2.4 Data Extraction, Quality Assessment and Risk of Bias
Upon completion of the abstract and full-text screening, information relating to the study design, number of participants, study aims and main findings was extracted. The mean ± standard deviation of all outcome measures following the muscle-damage protocols at 24 h, 48 h, 72 h and 96 h post-exercise for the pre-conditioning and control groups were entered into a custom-built Excel sheet. For studies where outcome measures were reported as figures, an e-mail requesting raw data was sent to corresponding authors. When a response was not provided by the corresponding authors, data from figures were extracted using a digitising software (ImageJ; National Institutes of Health, Bethesda, MD, USA). The methodological quality of each study was assessed using the Kmet appraisal checklist for quantitative studies [31]. The Kmet scoring tool consists of a three-point ordinal scoring system (‘yes’ = 2, ‘partial’ = 1, ‘no’ = 0), with appropriate validity and reproducibility [31]. Given that several of the Kmet criteria were inapplicable for the distinct study designs employed by the included studies, these criteria were either modified or replaced, with potential confounding variables common within the study design of EIMD studies. Specifically, the scores for criterion 4 (subject characteristics or input variables/information sufficiently described, additional scoring considerations for section) were modified to the following: a score of 2 if participants were clearly described as ‘untrained’ for more than 6 months and criteria for inclusion regarding training history were clearly outlined; a score of 1 if participants were described as ‘untrained’ but criteria for inclusion regarding training history were not clearly outlined; and a score of 0 if the participant’s training history was not clearly defined or participants were trained with no cessation period prior to study commencement. Criterion 5 (if random allocation to a treatment group was possible, is it described?) was modified to the following: a score of 2 if participants were matched by MVC or another appropriate baseline measure and randomised with the description of the method used; a score of 1 if participants were matched by MVC or other criteria but not randomised, or a method of randomisation was not mentioned; a score of 0 if participant allocation to a group was not clearly described. Criterion 6 (interventional and blinding of investigators to intervention was possible, is it reported?) was modified to the following: if baseline or pre-test measures included eccentric or isometric contractions, was a washout period observed prior to treatment commencing? A score of 2 if adequate time was allocated to allow for the cessation of any RBE occurring from the contraction present in the study; a score of 1 if concentric contractions were measured only, some time may be present between testing and treatment; a score of 0 if eccentric or isometric contractions were present and time allocated between baseline or pre-test measures not adequate to extinguish a repeated bout effect. Criterion 7 (If interventional and blinding of subjects to intervention was possible is it reported?) was modified to the following: were measures of dependent variables taken at the same time of day or within a specified window? A score of 2 if the time of day that dependent variables were measured was specified in the methodology (or elsewhere in the study); a score of 1 if the time of day was not specified but a similar time of day could be assumed based on evidence elsewhere, for example, figures or tables; a score of 0 if the time of day was not specified in the methodology and cannot be assumed based on other information present in study. Criteria 12. (Controlled for confounding?) were modified to: were dependent variables recorded at appropriate intervals? A score of 2 if dependent variables were measured daily with no less than 2 consecutive days post-intervention; a score of 1 if dependent variables were measured at regular intervals but may skip some 24-h periods; a score of 0 if dependent variables were measured randomly with no reasoning behind the schedule. Individual scores were reported for each study using an equation [31], and overall scores of < 50, 50–66, 67–82 and > 82 were expressed as ‘poor’, ‘fair’, ‘good’ and ‘excellent’ [32], respectively. The certainty of evidence was also assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE).
2.5 Certainty of Evidence
The certainty of evidence for each outcome was examined by two authors (KD and US) using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) protocol with ratings that ranged from very low to high levels of certainty [33,34,35]. The evidence was downgraded based on the following reasons: (i) risk of bias in studies: downgraded if the average Kmet scores were fair (< 67%) or by two levels if they were poor (< 50%); (ii) indirectness: a low risk of indirectness was caused because of the specificity of populations, interventions, comparators and outcomes being guaranteed by the eligibility criteria; (iii) a risk of publication bias: the judgements were downgraded by one level if there was a publication bias; (iv) inconsistency: downgraded by one level if the interstudy heterogeneity (I2) was high (> 75%); and (v) imprecision: downgraded by one level when < 800 participants were available [36].
2.6 Statistical Analysis
A meta-analysis was conducted to determine the effectiveness of pre-conditioning strategies for EIMD prevention using the RevMan (version 5.4) statistical software (2020; The Nordic Cochrane Centre, Copenhagen, Denmark). All outcome measures of interest relating to EIMD (CK, DOMS, ROM and muscular contractility) from each study were reported as mean ± standard deviation. The outcome measures were compared between the control group (no pre-conditioning) and pre-conditioning group at 24 h, 48 h, 72 h and 96 h after the muscle-damaging protocol. For studies where a control group was not included, the group that performed equivalent exercises between pre-conditioning (i.e. first bout) and the subsequent muscle-damaging protocol (i.e. second bout) was treated as the control group. For example, in the study by Nosaka et al. [18], participants were separated into three separate groups that performed two maximal eccentric contractions (2ECC), six maximal eccentric contractions (6ECC) or 24 maximal eccentric contractions (24ECC) as pre-conditioning exercises (i.e. first bout). All the participants then performed 24 maximal eccentric contractions 2 weeks later as their muscle-damaging protocol (i.e. second bout). In this instance, we extracted data following the pre-conditioning activity (i.e. first bout) for the 24ECC group and treated these data as our control group. The data extracted following the muscle-damaging exercises (i.e. bout 2) from 2 and 6ECC were treated as the pre-conditioning groups in our meta-analysis. Once all data were extracted from each study, forest plots were generated to determine differences between groups using the random-effects model. The magnitude of differences (i.e. pre-conditioning vs control groups) was calculated based on standardised mean differences, with values of 0.2, 0.5 and 0.8 considered small, medium and large, respectively. The between-group differences based on the pooled data were quantified as Z-values from the forest plot, in conjunction with p-values to determine the level of statistical significance, and the alpha level set at 0.05. Thus, effectiveness of the pre-conditioning activities was ascertained according to standardised mean differences and statistical significance between the pre-conditioning and control groups. The heterogeneity of the data points was assessed using I2 statistics, with values of 25%, 50% and 75% classified as low, moderate and high, respectively. To determine a potential publication bias, Egger’s test was conducted using the Statistical Package of Social Sciences (SPSS, version 26; IBM, Corporation, Armonk, NY, USA).
3 Results
3.1 Systematic Literature Search
A total of 5803 abstracts were extracted and screened according to the inclusion criteria from PubMed, Scopus and CINAHL databases. Following screening, 5742 abstracts were excluded, and the remaining 61 full-text articles were further assessed, leaving 23 articles for inclusion (Fig. 1).
3.2 Outcome Measures
Primary outcome measures included in the current review were common measures associated with EIMD; biochemical markers, physical performance, post-exercise muscle soreness, swelling and degrees of joint motion. These measures have previously been used as strong indicators of EIMD. Biochemical markers of indirect muscle damage included CK and myoglobin, whilst physical performance measures included MVC, maximal isometric torque, peak isometric force, peak eccentric force, peak concentric force and maximal eccentric contraction. Post-exercise muscle soreness was classified based on a subjective rating of muscle soreness using visual analogue scales. Swelling was measured externally by measuring the girth circumference in millimetres of the affected limb segment. Degrees of joint motion were taken as the percentage of change in degrees of the affected limb, or a true change in degrees, symptomatic of reduced contractility and tissue swelling.
3.3 Participants
Studies that included all groups with pre-conditioning activities had a total sample size of 427 participants (Table 1). The average age, height and body mass (including range) for isometric pre-conditioning and ECC pre-conditioning groups were 20.3 years (21–70 years), 164 cm (159–178 cm) and 62.4 kg (58–89 kg), respectively. Similar characteristics were present for studies with those that had a control group (i.e. no pre-conditioning activity), for which the total sample size was 261 participants with an average age, height and body mass (including range) of 22.1 years (20–30 years), 160 cm (159–187 cm) and 71.4 kg (50–91 kg). When baseline measures were compared between the isometric pre-conditioning and ECC pre-conditioning groups across both study designs, no significant differences were identified (p > 0.05), indicating between-group measures were relatively homogenous.
3.4 Methodological Descriptions
For the research design, 11 studies included a control group with no pre-conditioning activities, whilst eight studies incorporated groups where all participants performed pre-conditioning activities. Various types of interventions were used as pre-conditioning strategies to prevent EIMD (Table 2), with the most common being low-intensity or low-volume eccentric contractions (11 studies), followed by maximal isometric contractions (six studies), Smith machine squatting (one study), and downhill or level walking (one study). One study used both isometric and eccentric contractions as pre-conditioning, whilst one study used maximal isometric and eccentric contractions in separate groups. A variety of exercises were used to cause EIMD (Table 2), with the most common being eccentric contractions (15 studies) followed by downhill running (two studies), downhill walking (one study) and squatting (one study). The most common biomarkers for indirect muscle damage were CK (18) and myoglobin (10). One study did not measure blood biomarkers of EIMD. The level of DOMS was reported by 19 studies using visual analogue scales of 1–10, 1–100 or 1–200, with greater ratings indicating higher perceived soreness. Muscle swelling was reported using upper arm girth (eight studies), thigh girth (two studies) and ultrasound (six studies). Physical performance was measured using MVC of either the elbow flexors or knee extensors (eight studies), MVC torque of either the elbow or knee extensors (ten studies), running economy (one study) and 3-km time trial (one study). In addition, 11 studies examined ROM of the elbow joint or knee joint. Time between pre-conditioning and muscle damaging protocols varied among studies; some studies utilised more than one time period between groups. The most common durations between pre-conditioning and muscle-damaging protocols were 2 days (eight studies), 2 weeks (eight studies), 1 week (six studies) and 3 weeks (five studies).
3.5 Methodological Quality and Risk of Bias
The Kmet values for included studies ranged from good to excellent (Table 3). All included studies met the following criteria: eligibility criteria; similar measures at baseline and days 1–4; participants shared a similar training background; use of a pre-conditioning protocol; EIMD protocol performed more than 24 h after pre-conditioning; reported two or more outcome measures associated with EIMD (e.g. CK, myoglobin, ROM, MVC, DOMS or muscle girth); and results reported with measures of central tendency and dispersion. According to Egger’s test, all parameters at each time point were statistically significant (p < 0.05), indicating a publication bias.
3.6 Quantitative Analysis
The pre-conditioning groups demonstrated significantly lower CK levels than EIMD-only groups at 24 h (SMD = − 1.42; Z = 8.00; p = 0.00001), 48 h (SMD = − 2.21; Z = 9.50; p = 0.00001), 72 h (SMD = − 2.21; Z = 9.50; p = 0.00001) and 96 h post-exercise (SMD = − 3.22; Z = 9.57; p = 0.00001). In addition, substantial inter-study heterogeneity was identified for CK at 24 h (I2 = 82%; \(\chi^{2}\) = 219.0), 48 h (I2 = 88%; \(\chi^{2}\) = 345.8), 72 h (I2 = 87%; \(\chi^{2}\) = 283.0) and 96 h (I2 = 91%; \(\chi^{2}\) = 418.5) [Electronic Supplementary Material (ESM)]. Similarly, DOMS was significantly lower in the pre-conditioning groups than EIMD only groups at 24 h (SMD = − 1.94; Z = 8.27; p = 0.00001), 48 h (SMD = − 2.52; Z = 10.50; p = 0.00001), 72 h (SMD = − 2.70; Z = 10.61; p = 0.00001) and 96 h post-exercise (SMD = − 2.21; Z = 9.99; p = 0.00001), with substantial inter-study heterogeneity at 24 h (I2 = 89%; \(\chi^{2}\) = 416.7), 48 h (I2 = 89%; \(\chi^{2}\) = 405.9), 72 h (I2 = 89%; \(\chi^{2}\) = 392.0) and 96 h (I2 = 89%; \(\chi^{2}\) = 379.7) [ESM]. The pre-conditioning groups maintained MVC and returned to pre EIMD levels sooner than the EIMD-only groups at 24 h (SMD = 1.47; Z = 6.85; p = 0.00001), 48 h (SMD = 1.63; Z = 7.26; p = 0.00001), 72 h (SMD = 1.99; Z = 7.48; p = 0.00001) and 96 h post-exercise (SMD = 2.11; Z = 6.36; p = 0.00001), with substantial inter-study heterogeneity identified for MVC at 24 h (I2 = 82%; \(\chi^{2}\) = 147.6), 48 h (I2 = 81%; \(\chi^{2}\) = 148.3), 72 h (I2 = 86%; \(\chi^{2}\) = 197.4) and 96 h (I2 = 89%; \(\chi^{2}\) = 185.9) [ESM]. Finally, the pre-conditioning groups better maintained ROM after EIMD compared with EIMD-only groups at 24 h (SMD = 1.43; Z = 5.89; p = 0.00001), 48 h (SMD = 2.05; Z = 7.50; p = 0.00001), 72 h (SMD = 2.52; Z = 7.79; p = 0.00001) and 96 h post-exercise (SMD = 2.43; Z = 7.65; p = 0.00001), with substantial inter-study heterogeneity present at 24 h (I2 = 86%; \(\chi^{2}\) = 201.4), 48 h (I2 = 88%; \(\chi^{2}\) = 236.4), 72 h (I2 = 90%; \(\chi^{2}\) = 272.4) and 96 h (I2 = 90%; \(\chi^{2}\) = 290.1) [ESM].
3.7 Qualitative Analysis
3.7.1 Level of Protection from EIMD from Various Pre-Conditioning Protocols
When examining individual studies that compared various pre-conditioning protocols, the contraction type, intensity, volume, and joint angle of pre-conditioning activities and the duration between pre-conditioning activities and the muscle-damaging protocol appeared to influence the magnitude of protection from EIMD following subsequent muscle-damaging exercises. For example, with respect to the duration between pre-conditioning activities and the EIMD protocol, significantly lower EIMD was reported when the pre-conditioning activities (30 eccentric contractions at 10% MVC of elbow [21] and knee [23] flexors, two repetitions of MVC of elbow flexors [15]) were performed 2–4 days before the muscle-damaging exercises when compared with the pre-conditioning activities performed 1–3 weeks before the muscle-damaging exercises [21, 23] and immediately before the muscle-damaging protocol [15]. With respect to the volume of pre-conditioning activities, a greater volume of the pre-conditioning activity performed before the muscle-damaging exercises also exhibited lower levels of EIMD, such as the comparison between 10 repetitions of MVC to two repetitions of MVC held for 3 s during each MVC [10] and six eccentric contractions to two eccentric contractions [18]. However, results from one study showed no differences in the level of EIMD between pre-conditioning activities of 10 and 30 eccentric contractions [28]. Pre-conditioning activities performed with higher intensity showed lower levels of EIMD following muscle-damaging exercises, such as the comparison between 30 eccentric contractions performed at 80% of MVC to 40% and 60% of MVC, although no differences were found between 40 and 60% of MVC [2]. Furthermore, the level of EIMD was lower with pre-conditioning activities of 30 eccentric contractions performed at 20% of MVC than with 10% of MVC before the muscle-damaging exercises [38]. Interestingly, when comparing these two studies based on our forest plots, the SMD values were relatively similar for 30 eccentric contractions performed at 10–20% of MVC [38] and 40–60% of MVC [2] for CK, DOMS and MVC measures (ESM), although lower EIMD levels and a faster recovery of MVC were found with 30 eccentric contractions performed at 80% of MVC [2]. Downhill walking for 5 min also exhibited lower levels of EIMD as a pre-conditioning activity when compared with flat walking for 5 min [16], further supporting greater protection from EIMD with a higher intensity of pre-conditioning exercises. When comparing contraction types, eccentric contractions exhibited a greater protection from EIMD than isometric contractions [38]. Finally, pre-conditioning activities consisting of 30 repetitions of MVC held for 3 s during each contraction performed at an elbow angle of 20° (lengthened elbow flexors) showed greater protection from EIMD than at an elbow angle of 90° (shortened elbow flexors).
3.7.2 Level of EIMD After Various Pre-Conditioning Activities
When examining the acute responses to the pre-conditioning exercises, no significant differences in EIMD markers (i.e. CK, DOMS and MVC) were reported after 5 min of flat and downhill walking [16], 30 sub-maximal eccentric contractions of knee flexors and 60 eccentric contractions of knee extensors performed at 10% of MVC [23], 30 sub-maximal eccentric contractions at 10% MVC of elbow flexors [21] and two repetitions of MVC performed at 20° of an elbow flexion angle held for 3 s during each contraction [10, 15]. However, a significant increase in DOMS and a reduction in MVC were reported after 10 and 30 maximal eccentric contractions for at least 72 h post-exercise [28]. In addition, significant increases in CK and DOMS and a loss in MVC were reported after 30 sub-maximal eccentric contractions performed at 40%, 60% and 80% of MVC for at least 48-h post-exercise [2]. Furthermore, DOMS was significantly increased for 48 h and MVC was impaired for at least 24 h after 30 sub-maximal eccentric contractions at 10% and 20% of MVC, and 30 repetitions of MVC at 20° of an elbow flexion angle [38]. However, in the same study [38], DOMS was significantly increased, whilst MVC was decreased for only 24 h after 30 repetitions of MVC at 90° of an elbow flexion angle. Differences between baseline and post-exercise were not reported after the pre-conditioning activity for EIMD in one study [18], although CK and DOMS were notably increased for at least 48 h after 2 and 6 repetitions of maximal eccentric contractions, with 6 repetitions of maximal eccentric contractions exhibiting significantly greater EIMD than 2 maximal eccentric contractions.
3.8 Certainty of Evidence
The certainty of evidence for all outcomes (Table 4) was very low based primarily on the limited sample size for comparison (n < 800), publication bias and high inter-study heterogeneity (I2 > 75%).
4 Discussion
The current systematic review and meta-analysis examined the extent to which pre-conditioning interventions attenuate EIMD. Applying stringent inclusion criteria, 19 articles were included in the meta-analysis. Based on meta-analytical data, pre-conditioning interventions attenuated the level of EIMD (i.e. CK, DOMS, ROM and MVC) when performed a minimum of 24 h prior to a bout of strenuous exercise, compared with groups without pre-conditioning activities. In addition, the participants recovered from EIMD more quickly when exposed to pre-conditioning activities, with notably greater SMD values from 24 h post-exercise to 72 h post exercise. Furthermore, the pre-conditioning activities appeared to be most effective with the following: when implemented 2–4 days prior to the EIMD protocols; when pre-conditioning activities were performed with greater volume (10–30 eccentric contractions) compared to lower volume (2–6 eccentric contractions); when pre-conditioning activities were performed at higher intensities (20–80% of MVC) as opposed to lower intensities (10% MVC); when pre-conditioning activities were performed with more lengthened muscles; and eccentric contractions exhibited greater protection than isometric contractions. Whilst several of the pre-conditioning activities employed in these studies also increased the level of EIMD (elevated CK and DOMS and decreased MVC), the level of EIMD was notably lower than in the control group after the EIMD protocol. Thus, implementing pre-conditioning activities as a priming method prior to the initial exposure of muscle-damaging exercises alleviates symptoms of EIMD, and may accelerate recovery.
According to the traditional concept of RBE, a high level of EIMD is expected following the first bout of muscle-damaging exercises to minimise the level of EIMD following the second bout of similar, or identical muscle-damaging exercises [6, 11]. However, studies in this review achieved a similar prophylactic response to the RBE using pre-conditioning, bypassing the need for an initial high level of EIMD response. Pre-conditioning activities may provide an alternative with the benefits of the RBE that can be tailored for a specific outcome. A potent RBE brought about by traditional means of EIMD such as heavy strength training may attenuate subsequent muscle damage for months [2, 13]. However, the duration of protection from the pre-conditioning intervention appears to be specific to the type of intervention chosen, with low-volume maximal isometric pre-conditioning (IPC) utilising between two and ten isometric contractions attenuating muscle damage for only a few days (2–4 days) [10, 15, 17], while higher volume IPC appears to maintain attenuation potential for several weeks [13, 19].
The use of eccentric pre-conditioning has also been shown to maintain protective capacity against EIMD for weeks to months using low-volume maximal eccentric contractions to attenuate a second bout of high-volume ECC of the same exercise [18, 28]. Similar protective effects have been observed using sub-maximal intensity (10%) EPC to attenuate EIMD caused by a second damaging bout of high-volume and high-intensity ECC of the same exercise [13, 22]. The data in this review show that IPC interventions using between 2 and 60 isometric contractions provide adequate attenuation from CK, DOMS, ROM and MVC [10, 15, 19]. Similarly, EPC between 2 and 60 ECC contractions or sub-maximal ECC (10% MVC) also successfully attenuates EIMD [2, 10, 13, 22]. Both IPC and EPC can be applied in a range of scenarios and tailored to the specific needs of an individual’s programme where EIMD may not be desirable.
Several mechanisms have been proposed to explain how pre-conditioning activities attenuate muscle damage in the absence of any noticeable stimulus. Type IV collagen within the extracellular matrix (ECM) may interact with isometric and low-intensity ECC, allowing for a slow contraction of the type IV fibres. The alignment of ECM in this way may improve the transduction of force through the musculoskeletal system [43]. The slow contraction of the ECM may explain why EIMD will occur when exercise is completed immediately after pre-conditioning, although attenuated 24 h later. Furthermore, eccentric contractions as pre-conditioning activities have been suggested to upregulate the cytoskeletal proteins, which may strengthen the cytoskeletal protein network by stabilising the sarcomeres during eccentric contractions in subsequent muscle-damaging bouts [44]. It has also been suggested that pre-conditioning exercises may upregulate anti-oxidant enzymes whilst concomitantly reducing inflammatory markers, which may attenuate the secondary muscle damage response following subsequent muscle-damaging bouts [45, 46]. The duration of protection, particularly from maximal isometric contractions, is short lived, lasting only several days. It is therefore possible that non-damaging contractions may prevent EIMD by facilitating greater force output and muscle fibre recruitment as a result of familiarisation. In addition, muscle length appears to be an important factor in the success of a pre-conditioning strategy, as force production is greatly affected by muscle length afforded by the angle of a joint [47,48,49]. In the study by Chen et al. [38], 90° of elbow extension produced a less potent result than 20° of elbow extension during isometric contractions, highlighting the importance of muscle length when attempting pre-conditioning for EIMD. Ofori et al. [48] observed that muscle fibre recruitment and force production were affected by fibre length and ROM of the muscle being used, with force production greatest when muscle fibre length was long. This allowed for greater fibre recruitment while taking advantage of the mechanical and neural properties afforded by fibre elongation. The current meta-analysis exhibited significantly lower levels of EIMD for the pre-conditioning group from various interventions, suggesting that non-damaging protection against EIMD from subsequent strenuous training sessions is achievable using a variety of pre-conditioning strategies. However, the mechanisms offering protection are still debatable, and require more exploration beyond the scope of this review.
Several studies included in this review used sub-maximal isometric or concentric MVCs during familiarisation and baseline testing to reduce interference with the chosen pre-conditioning strategy [10, 13, 37]. While it is generally accepted that concentric contractions do not confer muscle damage at low volumes [1, 50], it remains unclear as to what extent concentric contractions affect the outcomes associated with EIMD. Similarly, the use of sub-maximal isometric contractions during familiarisation may have conferred some degree of pre-conditioning. Whilst this was not evident in the data within this review, the exploration of isometric thresholds that exhibit protection from EIMD may be valuable in broadening the application of pre-conditioning. Research implementing MVC and ECC as outcome measures should also consider how the implementation of MVC at baseline will impact their outcomes. The studies included in this review highlight that pre-conditioning can affect MVC, ROM and other measures of performance for up to 3 weeks, while some studies have shown that a single bout of ECC can have a RBE lasting several months [18]. This review corroborates suggestions made by Chen et al. [15] and Nosaka et al. [18] that studies examining the level of EIMD of an intervention should implement a washout period, allowing adequate time for interference from pre-testing and/or baseline measures to dissipate.
It is unclear exactly which pre-conditioning strategies would be effective for use prior to athletic performance. However, based on data collected from this review, it is possible to speculate that pre-conditioning may attenuate EIMD resulting from strenuous training. Similarly, pre-conditioning may improve concurrent training outcomes. Pre-conditioning could be implemented into periodisation plans to reduce EIMD between training sessions, improving the quality of cardiovascular training that occurs post-resistance training, particularly for endurance athletes for whom resistance training is less frequent or when commencing resistance training after a break or as part of a new training regime. This would ultimately lead to greater training quality, allowing full ROM and force production while reducing the injury risk during training for endurance athletes [16, 20].
The complex nature of sporting competition makes speculation regarding the effectiveness and appropriate application of pre-conditioning for athletes challenging. Further evaluation is therefore required to explore the use and effectiveness of pre-conditioning in sport. Many studies in this review utilised mono-articular pre-conditioning interventions. Mono-articular movement does not replicate the complexity of most training exercises, utilising only a single joint and only the muscles that cross that joint. Multi-articular pre-conditioning offers a greater opportunity for pre-conditioning to transfer to the real world, using multiple joints and muscles working at varying angles across an entire limb [19, 20, 22]. Lima et al. [20] implemented multi-articular isometric contractions using a leg press machine followed by a bout of downhill running. The EIMD induced by downhill running was attenuated by the isometric leg press as measured by CK, MVC and muscle soreness; however, running kinematics and metabolism were not significantly different between groups. This suggests the prophylactic effects of pre-conditioning can be transferred across different exercises if the same muscle groups are targeted. No studies included in this review implemented multiple exercises targeting the same muscle group in their second bout designed to cause EIMD. Traditional resistance training sessions typically consist of multiple exercises with a focus on developing a particular athletic attribute (power, strength, strength endurance). Huang et al. [22] did use multiple exercises to assess if EIMD could be attenuated by more than one muscular group; however, each exercise was preceded by a pre-conditioning activity specific to that exercise (e.g. 5 sets of 10 repetitions at 10% ECC on the lat pull down machine, followed 48 h later by 5 sets of 10 repetitions at 80% ECC on the lat pull down machine). It therefore remains unclear to what extent EIMD will be attenuated by a multi-articular pre-conditioning activity following a bout of traditional resistance exercises that are performed with multi-articular activities.
During methodological quality assessment of studies in the current systematic review, several areas were identified as generally scoring low using the Kmet criteria. These include:
-
Method of subject selection: the majority of studies scored 1 in this area because of the lack of specificity regarding subjects' training history. Subjects were generally described as healthy, untrained or non-resistance trained in some capacity; however, these criteria were not always well defined and exclusion criteria were not always clear. Greater specificity regarding subject inclusion criteria is necessary to ensure that a variation in participants' training volume or daily activities does affect the degree of protection afforded by pre-conditioning strategies.
-
If baseline or pre-test measures included eccentric or isometric contractions, was a washout period observed prior to treatment commencing: many studies scored a 0 or 1 in this area, as there was either no washout period observed or it was unclear when pre-testing took place prior to intervention. If a washout period is not considered before the intervention, any response will be affected by pre-test measures, thus confounding the EIMD response during the intervention. Future studies should implement a washout period prior to the intervention to allow for any pre-conditioning that occurs because of pre-testing to dissipate.
-
Dependent variables taken at the same time of day or within a specified window: many studies in this review scored a 1 on this item. The outcome measures of DOMS, MVC and CK are affected by the time of day and the duration between sessions, and as such, the specificity regarding subject attendance time is important. Many studies in this review included time points in tables and figures but did not specify if these measures were taken at approximately 24 h or within a window of time after 24 h. It is important that future studies are specific when participants attended consecutive sessions and within what window of time, as this may affect outcome measures.
It is unclear if pre-conditioning attenuates more than one bout of intense exercise performed over multiple days, and thus future research could examine the effectiveness of pre-conditioning exercises across multiple muscle-damaging bouts. Furthermore, future research should consider how isometric pre-conditioning can be implemented practically for athletes involved in concurrent training; identify at what thresholds isometric pre-conditioning provides attenuation; and determine whether isometric pre-conditioning can be used to attenuate muscle damage during multiple compound exercises such as those performed in a typical resistance training session. Such information would be useful for athletes during a high-load training phase or during intense competition phases. Finally, the type of pre-conditioning protocols and muscle-damaging protocols varied between studies, which may have affected the severity of EIMD. Eccentric exercise is an effective pre-conditioning strategy for attenuating muscle damage; however, this type of contraction produces some level of muscle damage as evidenced by previous studies [2, 18, 28].
The variation in pre-conditioning strategies included was a limitation of the current review, particularly the variation in pre-conditioning intensity amongst eccentric-based interventions, which possibly contributed to high inter-study heterogeneity in most cases (I2 > 75%). A further limitation of the review was that studies were combined with varying timing between pre-conditioning and the second bout of damaging exercise, different muscle groups (upper body vs lower body) and contraction types (isometric vs eccentric) into our meta-analyses. Although the current meta-analysis indicated that pre-conditioning activities reduce the level of EIMD following subsequent EIMD bouts, it is important to note that publication bias was present in all outcome measures, and the certainty of evidence was low. Finally, whilst every effort was made to contact the authors of each paper, most data were extracted from figures using data extracting software (ImageJ), which may result in some variation from the original results of each paper.
5 Conclusions
The current systematic review identified that pre-conditioning activities are effective in attenuating EIMD measures, CK, muscle soreness, ROM and maximal voluntary force production. These findings suggest the use of pre-conditioning activities prior to a strenuous bout of exercise does provide a significant protective effect when performed a minimum of 24 h prior to the damaging stimulus. Furthermore, the greater improvement in MVC suggests that the pre-conditioning activities may accelerate the recovery of muscle contractile properties following strenuous exercises. However, it is unclear if pre-conditioning would prevent EIMD from more complex exercises or to what extent EIMD prevention carries over into other modes of exercise.
References
Isner-Horobeti M-E, Dufour SP, Vautravers P, Geny B, Coudeyre E, Richard R. Eccentric exercise training: modalities, applications and perspectives. Sports Med. 2013;43(6):483–512.
Chen TC, Nosaka K, Sacco P. Intensity of eccentric exercise, shift of optimum angle, and the magnitude of repeated-bout effect. J Appl Physiol (1985). 2007;102(3):992–9.
Eston RG, Finney S, Baker S, Baltzopoulos V. Muscle tenderness and peak torque changes after downhill running following a prior bout of isokinetic eccentric exercise. J Sports Sci. 1996;14(4):291–9.
Hyldahl RD, Hubal MJ. Lengthening our perspective: morphological, cellular, and molecular responses to eccentric exercise. Muscle Nerve. 2014;49(2):155–70.
Doma K, Deakin GB, Bentley DJ. Implications of impaired endurance performance following single bouts of resistance training: an alternate concurrent training perspective. Sports Med. 2017;47(11):2187–200.
Doma K, Deakin GB, Schumann M, Bentley DJ. Training considerations for optimising endurance development: an alternate concurrent training perspective. Sports Med. 2019;49(5):669–82.
Maeo S, Ochi Y, Yamamoto M, Kanehisa H, Nosaka K. Effect of a prior bout of preconditioning exercise on muscle damage from downhill walking. Appl Physiol Nutr Metab. 2015;40(3):274–9.
Nosaka K, Clarkson PM. Influence of previous concentric exercise on eccentric exercise-induced muscle damage. J Sports Sci. 1997;15(5):477–83.
Nosaka K, Sakamoto K, Newton M, Sacco P. How long does the protective effect on eccentric exercise-induced muscle damage last? Med Sci Sports Exerc. 2001;33(9):1490–5.
Chen HL, Nosaka K, Pearce AJ, Chen TC. Two maximal isometric contractions attenuate the magnitude of eccentric exercise-induced muscle damage. Appl Physiol Nutr Metab. 2012;37(4):680–9.
Doma K, Schumann M, Leicht AS, Heilbronn BE, Damas F, Burt D. The repeated bout effect of traditional resistance exercises on running performance across 3 bouts. Appl Physiol Nutr Metab. 2017;42(9):978–85.
Doma K, Schumann M, Sinclair WH, Leicht AS, Deakin GB, Hakkinen K. The repeated bout effect of typical lower body strength training sessions on sub-maximal running performance and hormonal response. Eur J Appl Physiol. 2015;115(8):1789–99.
Chen TC, Tseng WC, Huang GL, Chen HL, Tseng KW, Nosaka K. Low-intensity eccentric contractions attenuate muscle damage induced by subsequent maximal eccentric exercise of the knee extensors in the elderly. Eur J Appl Physiol. 2013;113(4):1005–15.
Lavender AP, Nosaka K. A light load eccentric exercise confers protection against a subsequent bout of more demanding eccentric exercise. J Sci Med Sport. 2008;11(3):291–8.
Chen TC, Chen HL, Lin MJ, Chen CH, Pearce AJ, Nosaka K. Effect of two maximal isometric contractions on eccentric exercise-induced muscle damage of the elbow flexors. Eur J Appl Physiol. 2013;113(6):1545–54.
Maeo S, Yamamoto M, Kanehisa H, Nosaka K. Prevention of downhill walking-induced muscle damage by non-damaging downhill walking. PLoS ONE. 2017;12(3): e0173909.
Barreto RV, de Lima LCR, Greco CC, Denadai BS. Protective effect conferred by isometric preconditioning against slow- and fast-velocity eccentric exercise-induced muscle damage. Front Physiol. 2019;10:1203.
Nosaka K, Sakamoto K, Newton M, Sacco P. The repeated bout effect of reduced-load eccentric exercise on elbow flexor muscle damage. Eur J Appl Physiol. 2001;85(1–2):34–40.
Tseng KW, Tseng WC, Lin MJ, Chen HL, Nosaka K, Chen TC. Protective effect by maximal isometric contractions against maximal eccentric exercise-induced muscle damage of the knee extensors. Res Sports Med. 2016;24(3):243–56.
Lima LCR, Bassan NM, Cardozo AC, Goncalves M, Greco CC, Denadai BS. Isometric pre-conditioning blunts exercise-induced muscle damage but does not attenuate changes in running economy following downhill running. Hum Mov Sci. 2018;60:1–9.
Chen HL, Nosaka K, Chen TC. Muscle damage protection by low-intensity eccentric contractions remains for 2 weeks but not 3 weeks. Eur J Appl Physiol. 2012;112(2):555–65.
Huang MJ, Nosaka K, Wang HS, Tseng KW, Chen HL, Chou TY, et al. Damage protective effects conferred by low-intensity eccentric contractions on arm, leg and trunk muscles. Eur J Appl Physiol. 2019;119(5):1055–64.
Lin MJ, Chen TC, Chen HL, Wu BH, Nosaka K. Low-intensity eccentric contractions of the knee extensors and flexors protect against muscle damage. Appl Physiol Nutr Metab. 2015;40(10):1004–11.
Vicky M, Ann VR, Nigel PG, Roger GE. Comparison of the symptoms of exercise-induced muscle damage after an initial and repeated bout of plyometric exercise in men and boys. J Appl Physiol. 2005;99(3):1174–81.
Vieira A, Blazevich A, Souza N, Celes R, Alex S, Tufano JJ, et al. Acute changes in muscle thickness and pennation angle in response to work-matched concentric and eccentric isokinetic exercise. Appl Physiol Nutr Metab. 2018;43(10):1069–74.
Warrior B, Blackwood DJ, Larson DJ, Black CD, Larson RD. Pennation angle of the quadricep femoris muscles in resistance trained males vs. non-resistance trained males: 326 Board #164 May 29 11:00 AM - 12:30 PM. Med Sci Sports Exerc. 2019;51(6 Suppl):81.
Ho CC, Nosaka K, Tseng KW, Tseng WC, Lau WY, Bogdanis GC, et al. Effect of preconditioning exercise on biceps brachii myotendinous junction displacement during elbow flexor eccentric exercise. Scand J Med Sci Sports. 2021;31(4):813–25.
Brown SJ, Child RB, Day SH, Donnelly AE. Exercise-induced skeletal muscle damage and adaptation following repeated bouts of eccentric muscle contractions. J Sports Sci. 1997;15(2):215–22.
Lima LC, Denadai BS. Attenuation of eccentric exercise-induced muscle damage conferred by maximal isometric contractions: a mini review. Front Physiol. 2015;6:300.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;29(372): n71.
Kmet LM, Cook LS, Lee RC. Standard quality assessment criteria for evaluating primary research papers from a variety of fields. In: Alberta Heritage Foundation for Medical Research. Alberta, Canada; 2004. p. 13.
Simmons R, Doma K, Sinclair W, Connor J, Leicht A. Acute effects of training loads on muscle damage markers and performance in semi-elite and elite athletes: a systematic review and meta-analysis. Sports Med. 2021;51(10):2181–207.
Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al. GRADE guidelines: 1. Introduction: GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64(4):383–94.
Zhang Y, Alonso-Coello P, Guyatt GH, Yepes-Nunez JJ, Akl EA, Hazlewood G, et al. GRADE guidelines: 19. Assessing the certainty of evidence in the importance of outcomes or values and preferences: risk of bias and indirectness. J Clin Epidemiol. 2019;111:94–104.
Zhang Y, Coello PA, Guyatt GH, Yepes-Nunez JJ, Akl EA, Hazlewood G, et al. GRADE guidelines: 20. Assessing the certainty of evidence in the importance of outcomes or values and preferences-inconsistency, imprecision, and other domains. J Clin Epidemiol. 2019;111:83–93.
Guyatt G, Oxman AD, Kunz R, Brozek J, Alonso-Coello P, Rind D, et al. Corrigendum to GRADE guidelines 6. Rating the quality of evidence-imprecision. J Clin Epidemiol. 2011;64:1283–93 (J Clin Epidemiol. 2021 Sep;137:265).
Burt D, Lamb K, Nicholas C, Twist C. Lower-volume muscle-damaging exercise protects against high-volume muscle-damaging exercise and the detrimental effects on endurance performance. Eur J Appl Physiol. 2015;115(7):1523–32.
Chen TC, Chen HL, Pearce AJ, Nosaka K. Attenuation of eccentric exercise-induced muscle damage by preconditioning exercises. Med Sci Sports Exerc. 2012;44(11):2090–8.
Howatson G, Van Someren K, Hortobagyi T. Repeated bout effect after maximal eccentric exercise. Int J Sports Med. 2007;28(7):557–63.
Paddon-Jones D, Abernethy PJ. Acute adaptation to low volume eccentric exercise. Med Sci Sports Exerc. 2001;33(7):1213–9.
Miyama M, Nosaka K. Protection against muscle damage following fifty drop jumps conferred by ten drop jumps. J Strength Cond Res. 2007;21(4):1087.
Nosaka K, Newton M, Sacco P, Chapman D, Lavender A. Partial protection against muscle damage by eccentric actions at short muscle lengths. Med Sci Sports Exerc. 2005;37(5):746–53.
Schleip R, Klingler W. Active contractile properties of fascia. Clin Anat. 2019;32(7):891–5.
Koh TJ, Brooks SV. Lengthening contractions are not required to induce protection from contraction-induced muscle injury. Am J Physiol Regul Integr Comp Physiol. 2001;281(1):R155–61.
McArdle F, Spiers S, Aldemir H, Vasilaki A, Beaver A, Iwanejko L, et al. Preconditioning of skeletal muscle against contraction-induced damage: the role of adaptations to oxidants in mice. J Physiol. 2004;561(Pt 1):233–44.
Pizza FX, Koh TJ, McGregor SJ, Brooks SV. Muscle inflammatory cells after passive stretches, isometric contractions, and lengthening contractions. J Appl Physiol (1985). 2002;92(5):1873–8.
Dick TJM, Wakeling JM. Shifting gears: dynamic muscle shape changes and force-velocity behavior in the medial gastrocnemius. J Appl Physiol (1985). 2017;123(6):1433–42.
Ofori E, Shim J, Sosnoff JJ. The influence of lower leg configurations on muscle force variability. J Biomech. 2018;71:111–8.
Rassier DE, MacIntosh BR, Herzog W. Length dependence of active force production in skeletal muscle. J Appl Physiol. 1999;86(5):1445–57.
Cheung K, Hume PA, Maxwell L. Delayed onset muscle soreness: treatment strategies and performance factors. Sports Med. 2003;33(2):145–64.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions. No sources of funding were used to assist in the preparation of this review.
Conflicts of Interest/Competing Interests
Lachlan Boyd, Glen Deakin, Baily Devantier-Thomas, Utkarsh Singh and Kenji Doma have no conflicts of interest that are directly relevant to the content of this review.
Ethics Approval
Not applicable.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Availability of Data and Material
Data will be provided upon request.
Code Availability
Not applicable.
Authors’ Contributions
LB, GBD and KD conceived the idea; LB and KD wrote the manuscript; LB, BDT and US screened the abstracts and full text; LB and BDT conducted the quality assessment; LB and BDT extracted data from the studies; US checked the accuracy of the data extraction; LB and US conducted the meta-analysis; GBD and KD interpreted the quantitative analyses; US assessed for a risk of bias and compiled the certainty of evidence; LB drafted the manuscript; GBD, BDT, US and KD critically revised the manuscript for important intellectual content; and GBD, BDT, US and KD approved the version to be published.
Supplementary Information
Below is the link to the electronic supplementary material.
40279_2023_1839_MOESM1_ESM.eps
Supplementary file 1. Forest plots effect of pre-conditioning on creatine kinases release 24 hours post damaging stimulus
40279_2023_1839_MOESM2_ESM.eps
Supplementary file 2. Forest plots effect of pre-conditioning on creatine kinases release 48 hours post damaging stimulus
40279_2023_1839_MOESM3_ESM.eps
Supplementary file 3. Forest plots effect of pre-conditioning on creatine kinases release 72 hours post damaging stimulus
40279_2023_1839_MOESM5_ESM.eps
Supplementary file 5. Forest plots showing effect of pre-conditioning on delayed onset muscle soreness 24 hours post damaging stimulus
40279_2023_1839_MOESM6_ESM.eps
Supplementary file 6. Forest plots showing effect of pre-conditioning on delayed onset muscle soreness 48 hours post damaging stimulus
40279_2023_1839_MOESM7_ESM.eps
Supplementary file 7. Forest plots showing effect of pre-conditioning on delayed onset muscle soreness 72 hours post damaging stimulus
40279_2023_1839_MOESM8_ESM.eps
Supplementary file 8. Forest plots showing effect of pre-conditioning on delayed onset muscle soreness 96 hours post damaging stimulus
40279_2023_1839_MOESM9_ESM.eps
Supplementary file 9. Forest plots showing effect of pre-conditioning on maximal voluntary contractions 24 hours post damaging stimulus
40279_2023_1839_MOESM10_ESM.eps
Supplementary file 10. Forest plots showing effect of pre-conditioning on maximal voluntary contractions 48 hours post damaging stimulus
40279_2023_1839_MOESM11_ESM.eps
Supplementary file 11. Forest plots showing effect of pre-conditioning on maximal voluntary contractions 72 hours post damaging stimulus
40279_2023_1839_MOESM12_ESM.eps
Supplementary file 12. Forest plots showing effect of pre-conditioning on maximal voluntary contractions 96 hours post damaging stimulus
40279_2023_1839_MOESM13_ESM.eps
Supplementary file 13. Forest plots showing effect of pre-conditioning on range of motion 24 hours post damaging stimulus
40279_2023_1839_MOESM14_ESM.eps
Supplementary file 14. Forest plots showing effect of pre-conditioning on range of motion 48 hours post damaging stimulu
40279_2023_1839_MOESM15_ESM.eps
Supplementary file 15. Forest plots showing effect of pre-conditioning on range of motion 72 hours post damaging stimulus
40279_2023_1839_MOESM16_ESM.eps
Supplementary file 16. Forest plots showing effect of pre-conditioning on range of motion 96 hours post damaging stimulus
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Boyd, L., Deakin, G.B., Devantier-Thomas, B. et al. The Effects of Pre-conditioning on Exercise-Induced Muscle Damage: A Systematic Review and Meta-analysis. Sports Med 53, 1537–1557 (2023). https://doi.org/10.1007/s40279-023-01839-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-023-01839-8