JAMA Surgery ( IF 16.9 ) Pub Date : 2018-08-01 , DOI: 10.1001/jamasurg.2018.1607 Julia Kitz 1 , Emmanouil Fokas 2 , Tim Beissbarth 3 , Philipp Ströbel 1 , Christian Wittekind 4 , Arndt Hartmann 5 , Josef Rüschoff 6 , Thomas Papadopoulos 7 , Elisabeth Rösler 8 , Peter Ortloff-Kittredge 8 , Ulrich Kania 9 , Hans Schlitt 10 , Karl-Heinrich Link 11 , Wolf Bechstein 12 , Hans-Rudolf Raab 13 , Ludger Staib 14 , Christoph-Thomas Germer 15 , Torsten Liersch 16 , Rolf Sauer 17 , Claus Rödel 2 , Michael Ghadimi 16 , Werner Hohenberger 18 ,
|
Importance Previous retrospective studies have shown that surgical quality affects local control in rectal cancer..
Objective In this secondary end point analysis, we evaluated the prognostic effect of the total mesorectal excision (TME) plane in the CAO/ARO/AIO-04 phase 3 randomized clinical trial.
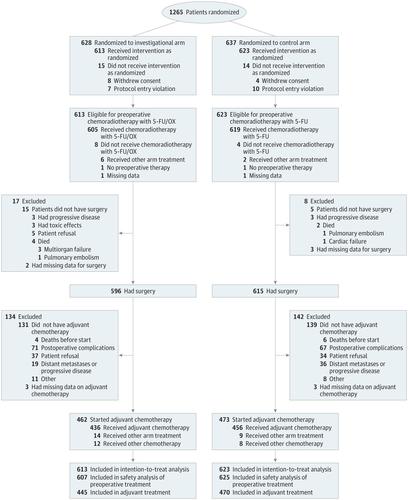
Design, Setting, and Participants The CAO/ARO/AIO-04 trial enrolled 1236 patients with cT3-4 and/or node-positive rectal adenocarcinoma from 88 centers in Germany between July 25, 2006, and February 26, 2010.
Interventions Patients were randomized to receive treatment with standard fluorouracil-based preoperative chemoradiotherapy (CRT) alone (control arm) or oxaliplatin (experimental arm) followed by TME and adjuvant chemotherapy.
Main Outcomes and Measures The TME quality (mesorectal, intramesorectal, and muscularis propria plane) was prospectively assessed in 1152 operation specimens. An assessment was performed independently by pathologists and surgeons. The results were correlated with clinicopathologic data and the clinical outcome was tested, including multivariable analysis with the Cox regression model.
Results Of 1152 German Caucasian participants, 332 (28.8) were women and the mean age was 63 years. The plane of TME was mesorectal in 930 patients (80.7%), intramesorectal in 169 (14.7%), and muscularis propria in 53 (4.6%). In a univariable analysis, the TME plane was significantly associated with 3-year disease-free survival (mesorectal vs intramesorectal vs muscularis propria, 95% CI, 73.1-78.8 vs 61.6-76.0 vs 55.6-81.3, respectively; P = .01), cumulative incidence of local and distant recurrences (mesorectal vs intramesorectal vs muscularis propria, 95% CI, 2.0-4.5 vs 1.2-8.1 vs 2.5-20.5, respectively; P < .001; and mesorectal vs intramesorectal vs muscularis propria, 95% CI, 17.0-22.4 vs 18.3-32.0 vs 14.2-39.0, respectively; P = .03, respectively), and overall survival (mesorectal vs intramesorectal vs muscularis propria, 95% CI, 88.3-92.3 vs 79.7-91.0 vs 81.6-98.7, respectively; P = .02). In contrast to the pathologist-based evaluation, the assessment of TME plane by the operating surgeon failed to demonstrate prognostic significance for any of these clinical end points. In a multivariable analysis, the plane of surgery (mesorectal vs muscularis propria TME) constituted an independent factor for local recurrence (P = .002).
Conclusions and Relevance This phase 3 randomized clinical trial confirms the long-term clinical effect of TME plane quality on local recurrence, as initially reported in the MRC CR07 study. The data highlight the key role of pathologists and surgeons in the multidisciplinary management of rectal cancer.
Trial Registration ClinicalTrials.gov Identifier: NCT00349076.
中文翻译:
全直肠系膜切除平面与直肠癌预后的关系CAO / ARO / AIO-04 3期随机临床试验的二级分析
重要性 以前的回顾性研究表明,手术质量会影响直肠癌的局部控制。
目的 在该次要终点分析中,我们评估了总直肠系膜切除(TME)平面在CAO / ARO / AIO-04 3期随机临床试验中的预后效果。
设计,背景和参与者 CAO / ARO / AIO-04试验从2006年7月25日至2010年2月26日在德国的88个中心招募了1236例cT3-4和/或淋巴结阳性的直肠腺癌患者。
干预措施 患者被随机分配接受标准的基于氟尿嘧啶的术前放化疗(CRT)或奥沙利铂(实验组),然后进行TME和辅助化疗。
主要结果和措施 前瞻性评估了1152例手术标本中的TME质量(大肠直肠,大肠直肠内和固有肌层)。评估由病理学家和外科医生独立进行。结果与临床病理数据相关,并测试了临床结局,包括使用Cox回归模型进行多变量分析。
结果 在1152名德国高加索参与者中,有332名(28.8)为女性,平均年龄为63岁。TME的平面为930例(80.7%)的直肠系膜,直肠内的169例(14.7%)的直肠系膜和53例(4.6%)的固有肌层。在单变量分析中,TME平面与3年无病生存率显着相关(大肠直肠与大肠直肠内与固有肌相比,95%CI,分别为73.1-78.8、61.6-76.0和55.6-81.3;P = 0.01) ,局部和远处复发的累积发生率(肠系膜vs直肠内膜vs固有肌层,分别为95%CI,2.0-4.5对1.2-8.1 vs 2.5-20.5;P <.001;以及直肠系膜对大肠直肠内相对于肌层固有体,95%CI ,分别为17.0-22.4、18.3-32.0和14.2-39.0;P 分别为.03)和总体生存率(大肠直肠vs.大肠直肠内vs.固有肌,95%CI,分别为88.3-92.3、79.7-91.0和81.6-98.7; P = .02)。与基于病理学家的评估相反,手术外科医生对TME平面的评估未能显示出对任何这些临床终点的预后意义。在多变量分析中,手术平面(直肠系膜vs固有肌层TME)构成局部复发的独立因素(P = .002)。
结论和相关 性正如MRC CR07研究最初报道的那样,该3期随机临床试验证实了TME平面质量对局部复发的长期临床效果。数据突出了病理学家和外科医生在直肠癌多学科管理中的关键作用。
试用注册 ClinicalTrials.gov标识符:NCT00349076。

























 京公网安备 11010802027423号
京公网安备 11010802027423号