JAMA Surgery ( IF 16.9 ) Pub Date : 2018-08-01 , DOI: 10.1001/jamasurg.2018.0985 Mark R. Hemmila 1 , Anne H. Cain-Nielsen 1 , Jill L. Jakubus 1 , Judy N. Mikhail 1 , Justin B. Dimick 1
|
Importance The American College of Surgeons Trauma Quality Improvement Program (ACS TQIP) provides feedback to hospitals on risk-adjusted outcomes. The Michigan Trauma Quality Improvement Program (MTQIP) goes beyond the provision of feedback alone, focusing on collaborative quality improvement. It is unknown whether the addition of a collaborative approach to benchmark reporting improves outcomes.
Objective To evaluate the association of hospital participation in the ACS TQIP (benchmark reporting) or the MTQIP (benchmark reporting and collaborative quality improvement) with outcomes compared with control hospitals that did not participate in either program.
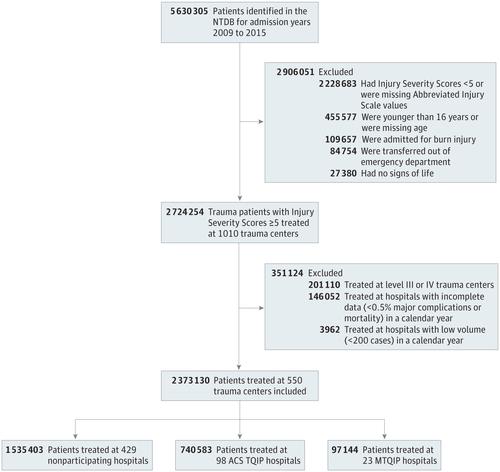
Design, Setting, and Participants In this cohort study, data from the National Trauma Data Bank from 2009 to 2015 were used. A total of 2 373 130 trauma patients 16 years or older with an Injury Severity Score of 5 or more were identified from 98 ACS TQIP hospitals, 23 MTQIP hospitals, and 429 nonparticipating hospitals, based on program participation status in 2011. A difference-in-differences analytic approach was used to evaluate whether hospital participation in the ACS TQIP or the MTQIP was associated with improved outcomes compared with nonparticipation in a quality improvement program.
Exposures Hospital participation in MTQIP, a quality improvement collaborative, compared with ACS TQIP participation and nonparticipating hospitals.
Main Outcomes and Measures In-hospital mortality, mortality or hospice, major complications, and venous thromboembolism events were assessed.
Results Of the 2 373 130 included trauma patients, 64.2% were men and 73.0% were white, and the mean (SD) age was 50.7 (21.9) years. After accounting for patient factors and preexisting time trends toward improved outcomes, there was a statistically significant improvement in major complications after (vs before) hospital enrollment in the MTQIP collaborative compared with nonparticipating hospitals (odds ratio [OR], 0.89; 95% CI, 0.83-0.95) or ACS TQIP hospitals (OR, 0.88; 95% CI, 0.82-0.94). A similar result was observed for venous thromboembolism (MTQIP vs nonparticipating: OR, 0.78; 95% CI, 0.69-0.88; MTQIP vs ACS TQIP: OR, 0.84; 95% CI, 0.74-0.95), for which MTQIP targeted specific performance improvement efforts. Hospital participation in both ACS TQIP and MTQIP was associated with improvement in mortality or hospice (ACS TQIP vs nonparticipating: OR, 0.90; 95% CI, 0.87-0.93; MTQIP vs nonparticipating: OR, 0.88; 95% CI, 0.81-0.96). Hospitals participating in MTQIP achieved the lowest overall risk-adjusted mortality in the postenrollment period (4.2%; 95% CI, 4.1-4.3).
Conclusions and Relevance This study demonstrates that hospital participation in a regional collaborative quality improvement program is associated with improved patient outcomes beyond benchmark reporting alone while promoting compliance with processes of care.
中文翻译:
医院参与区域创伤质量改善与患者结果的合作协会
重要性 美国外科医生学院创伤质量改进计划(ACS TQIP)向医院提供有关风险调整后结果的反馈。密歇根州创伤质量改进计划(MTQIP)不仅提供反馈,还致力于协作质量改进。尚不知道在基准报告中添加协作方法是否会改善结果。
目的 与没有参加该计划的对照医院相比,评估参与ACS TQIP(基准报告)或MTQIP(基准报告和协作质量改善)的医院与结局的相关性。
设计,背景和参与者 在本队列研究中,使用了国家创伤数据库(National Trauma Data Bank)2009年至2015年的数据。根据2011年的计划参与状态,从98 ACS TQIP医院,23 MTQIP医院和429非参与医院中,总共鉴定出2 373 130名16岁或以上的创伤严重程度得分在5以上的创伤患者。 -差异分析方法用于评估医院参加ACS TQIP或MTQIP是否与未参加质量改善计划相比改善了结局。
曝光 医院参与MTQIP,质量改进协作,与ACS TQIP参与和未参与的医院相比。
主要结果和措施评估了 院内死亡率,死亡率或临终关怀,主要并发症和静脉血栓栓塞事件。
结果 在2 373 130名外伤患者中,男性占64.2%,白人为73.0%,平均(SD)年龄为50.7(21.9)岁。在考虑了患者因素和已有的改善结果的时间趋势之后,与未参加调查的医院相比,MTQIP合作医院入院后(与之前相比)的主要并发症有统计学上的显着改善(优势比[OR]为0.89; CI为95%, 0.83-0.95)或ACS TQIP医院(OR为0.88; 95%CI为0.82-0.94)。对于静脉血栓栓塞也观察到了相似的结果(MTQIP与非参与性:OR,0.78; 95%CI,0.69-0.88; MTQIP与ACS TQIP:OR,0.84; 95%CI,0.74-0.95),针对MTQIP的特定性能改善努力。医院同时参与ACS TQIP和MTQIP与死亡率或临终关怀的改善相关(ACS TQIP与未参加者:或0.90;95%CI,0.87-0.93;MTQIP vs非参与:OR,0.88;95%CI,0.81-0.96)。参与MTQIP的医院在入组后的总体风险调整后死亡率最低(4.2%; 95%CI,4.1-4.3)。
结论与相关性 这项研究表明,医院参与区域协作质量改进计划不仅可以提高患者的治疗效果,而且可以提高对治疗过程的依从性,而不仅仅是基准报告。


























 京公网安备 11010802027423号
京公网安备 11010802027423号