Our official English website, www.x-mol.net, welcomes your feedback! (Note: you will need to create a separate account there.)
Effect of Bag-Mask Ventilation vs Endotracheal Intubation During Cardiopulmonary Resuscitation on Neurological Outcome After Out-of-Hospital Cardiorespiratory Arrest
JAMA ( IF 120.7 ) Pub Date : 2018-02-27 , DOI: 10.1001/jama.2018.0156 Patricia Jabre 1 , Andrea Penaloza 2 , David Pinero 3 , Francois-Xavier Duchateau 4 , Stephen W. Borron 5 , Francois Javaudin 6 , Olivier Richard 7 , Diane de Longueville 8 , Guillem Bouilleau 9 , Marie-Laure Devaud 10 , Matthieu Heidet 11 , Caroline Lejeune 12 , Sophie Fauroux 13 , Jean-Luc Greingor 14 , Alessandro Manara 15 , Jean-Christophe Hubert 16 , Bertrand Guihard 17 , Olivier Vermylen 18 , Pascale Lievens 19 , Yannick Auffret 20 , Celine Maisondieu 21 , Stephanie Huet 22 , Benoît Claessens 8 , Frederic Lapostolle 23 , Nicolas Javaud 24 , Paul-Georges Reuter 25 , Elinor Baker 23 , Eric Vicaut 26 , Frédéric Adnet 23
JAMA ( IF 120.7 ) Pub Date : 2018-02-27 , DOI: 10.1001/jama.2018.0156 Patricia Jabre 1 , Andrea Penaloza 2 , David Pinero 3 , Francois-Xavier Duchateau 4 , Stephen W. Borron 5 , Francois Javaudin 6 , Olivier Richard 7 , Diane de Longueville 8 , Guillem Bouilleau 9 , Marie-Laure Devaud 10 , Matthieu Heidet 11 , Caroline Lejeune 12 , Sophie Fauroux 13 , Jean-Luc Greingor 14 , Alessandro Manara 15 , Jean-Christophe Hubert 16 , Bertrand Guihard 17 , Olivier Vermylen 18 , Pascale Lievens 19 , Yannick Auffret 20 , Celine Maisondieu 21 , Stephanie Huet 22 , Benoît Claessens 8 , Frederic Lapostolle 23 , Nicolas Javaud 24 , Paul-Georges Reuter 25 , Elinor Baker 23 , Eric Vicaut 26 , Frédéric Adnet 23
Affiliation
|
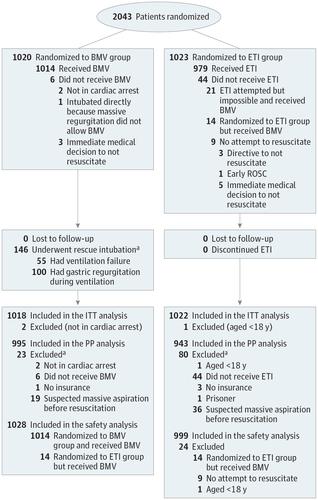
Importance Bag-mask ventilation (BMV) is a less complex technique than endotracheal intubation (ETI) for airway management during the advanced cardiac life support phase of cardiopulmonary resuscitation of patients with out-of-hospital cardiorespiratory arrest. It has been reported as superior in terms of survival. Objectives To assess noninferiority of BMV vs ETI for advanced airway management with regard to survival with favorable neurological function at day 28. Design, Settings, and Participants Multicenter randomized clinical trial comparing BMV with ETI in 2043 patients with out-of-hospital cardiorespiratory arrest in France and Belgium. Enrollment occurred from March 9, 2015, to January 2, 2017, and follow-up ended January 26, 2017. Intervention Participants were randomized to initial airway management with BMV (n = 1020) or ETI (n = 1023). Main Outcomes and Measures The primary outcome was favorable neurological outcome at 28 days defined as cerebral performance category 1 or 2. A noninferiority margin of 1% was chosen. Secondary end points included rate of survival to hospital admission, rate of survival at day 28, rate of return of spontaneous circulation, and ETI and BMV difficulty or failure. Results Among 2043 patients who were randomized (mean age, 64.7 years; 665 women [32%]), 2040 (99.8%) completed the trial. In the intention-to-treat population, favorable functional survival at day 28 was 44 of 1018 patients (4.3%) in the BMV group and 43 of 1022 patients (4.2%) in the ETI group (difference, 0.11% [1-sided 97.5% CI, −1.64% to infinity]; P for noninferiority = .11). Survival to hospital admission (294/1018 [28.9%] in the BMV group vs 333/1022 [32.6%] in the ETI group; difference, −3.7% [95% CI, −7.7% to 0.3%]) and global survival at day 28 (55/1018 [5.4%] in the BMV group vs 54/1022 [5.3%] in the ETI group; difference, 0.1% [95% CI, −1.8% to 2.1%]) were not significantly different. Complications included difficult airway management (186/1027 [18.1%] in the BMV group vs 134/996 [13.4%] in the ETI group; difference, 4.7% [95% CI, 1.5% to 7.9%]; P = .004), failure (69/1028 [6.7%] in the BMV group vs 21/996 [2.1%] in the ETI group; difference, 4.6% [95% CI, 2.8% to 6.4%]; P < .001), and regurgitation of gastric content (156/1027 [15.2%] in the BMV group vs 75/999 [7.5%] in the ETI group; difference, 7.7% [95% CI, 4.9% to 10.4%]; P < .001). Conclusions and Relevance Among patients with out-of-hospital cardiorespiratory arrest, the use of BMV compared with ETI failed to demonstrate noninferiority or inferiority for survival with favorable 28-day neurological function, an inconclusive result. A determination of equivalence or superiority between these techniques requires further research. Trial Registration clinicaltrials.gov Identifier: NCT02327026
中文翻译:

心肺复苏期间袋面罩通气与气管内插管对院外心肺骤停后神经功能结局的影响
重要性 在院外心肺骤停患者心肺复苏的高级心脏生命支持阶段,气囊面罩通气 (BMV) 是一种比气管内插管 (ETI) 更简单的气道管理技术。据报道,它在生存方面更胜一筹。目的 评估 BMV 与 ETI 在高级气道管理中在第 28 天神经功能良好的存活率方面的非劣效性。 设计、设置和参与者 多中心随机临床试验在 2043 名院外心肺骤停患者中比较 BMV 与 ETI法国和比利时。入组时间为 2015 年 3 月 9 日至 2017 年 1 月 2 日,随访截止日期为 2017 年 1 月 26 日。干预参与者随机接受 BMV(n = 1020)或 ETI(n = 1023)初始气道管理。主要结果和测量 主要结果是 28 天时的良好神经学结果,定义为大脑功能类别 1 或 2。选择了 1% 的非劣效性界限。次要终点包括入院生存率、第 28 天生存率、自主循环恢复率以及 ETI 和 BMV 困难或失败。结果 在随机分组的 2043 名患者(平均年龄 64.7 岁;665 名女性 [32%])中,2040 名 (99.8%) 完成了试验。在意向治疗人群中,BMV 组 1018 名患者中的 44 名 (4.3%) 和 ETI 组 1022 名患者中的 43 名 (4.2%) 在第 28 天良好的功能生存(差异,0.11% [单侧97.5% CI,-1.64% 至无穷大];非劣效性 P = .11)。入院存活率(BMV 组 294/1018 [28.9%] vs ETI 组 333/1022 [32.6%];差异,-3.7% [95% CI,-7.7% 至 0.3%])和第 28 天的总体生存率(BMV 组为 55/1018 [5.4%],而 ETI 组为 54/1022 [5.3%];差异) , 0.1% [95% CI, -1.8% 至 2.1%]) 没有显着差异。并发症包括气道管理困难(BMV 组为 186/1027 [18.1%],ETI 组为 134/996 [13.4%];差异,4.7% [95% CI,1.5% 至 7.9%];P = .004 ),失败(BMV 组为 69/1028 [6.7%],ETI 组为 21/996 [2.1%];差异,4.6% [95% CI,2.8% 至 6.4%];P < .001),和胃内容物反流(BMV 组 156/1027 [15.2%] vs ETI 组 75/999 [7.5%];差异,7.7% [95% CI,4.9% 至 10.4%];P < .001 )。结论和相关性 在院外心肺骤停患者中,与 ETI 相比,BMV 的使用未能证明在具有良好 28 天神经功能的生存方面具有非劣效性或劣势性,这是一个不确定的结果。确定这些技术之间的等效性或优越性需要进一步研究。试验注册clinicaltrials.gov 标识符:NCT02327026
更新日期:2018-02-27
中文翻译:
心肺复苏期间袋面罩通气与气管内插管对院外心肺骤停后神经功能结局的影响
重要性 在院外心肺骤停患者心肺复苏的高级心脏生命支持阶段,气囊面罩通气 (BMV) 是一种比气管内插管 (ETI) 更简单的气道管理技术。据报道,它在生存方面更胜一筹。目的 评估 BMV 与 ETI 在高级气道管理中在第 28 天神经功能良好的存活率方面的非劣效性。 设计、设置和参与者 多中心随机临床试验在 2043 名院外心肺骤停患者中比较 BMV 与 ETI法国和比利时。入组时间为 2015 年 3 月 9 日至 2017 年 1 月 2 日,随访截止日期为 2017 年 1 月 26 日。干预参与者随机接受 BMV(n = 1020)或 ETI(n = 1023)初始气道管理。主要结果和测量 主要结果是 28 天时的良好神经学结果,定义为大脑功能类别 1 或 2。选择了 1% 的非劣效性界限。次要终点包括入院生存率、第 28 天生存率、自主循环恢复率以及 ETI 和 BMV 困难或失败。结果 在随机分组的 2043 名患者(平均年龄 64.7 岁;665 名女性 [32%])中,2040 名 (99.8%) 完成了试验。在意向治疗人群中,BMV 组 1018 名患者中的 44 名 (4.3%) 和 ETI 组 1022 名患者中的 43 名 (4.2%) 在第 28 天良好的功能生存(差异,0.11% [单侧97.5% CI,-1.64% 至无穷大];非劣效性 P = .11)。入院存活率(BMV 组 294/1018 [28.9%] vs ETI 组 333/1022 [32.6%];差异,-3.7% [95% CI,-7.7% 至 0.3%])和第 28 天的总体生存率(BMV 组为 55/1018 [5.4%],而 ETI 组为 54/1022 [5.3%];差异) , 0.1% [95% CI, -1.8% 至 2.1%]) 没有显着差异。并发症包括气道管理困难(BMV 组为 186/1027 [18.1%],ETI 组为 134/996 [13.4%];差异,4.7% [95% CI,1.5% 至 7.9%];P = .004 ),失败(BMV 组为 69/1028 [6.7%],ETI 组为 21/996 [2.1%];差异,4.6% [95% CI,2.8% 至 6.4%];P < .001),和胃内容物反流(BMV 组 156/1027 [15.2%] vs ETI 组 75/999 [7.5%];差异,7.7% [95% CI,4.9% 至 10.4%];P < .001 )。结论和相关性 在院外心肺骤停患者中,与 ETI 相比,BMV 的使用未能证明在具有良好 28 天神经功能的生存方面具有非劣效性或劣势性,这是一个不确定的结果。确定这些技术之间的等效性或优越性需要进一步研究。试验注册clinicaltrials.gov 标识符:NCT02327026


























 京公网安备 11010802027423号
京公网安备 11010802027423号