当前位置:
X-MOL 学术
›
JAMA Pediatr.
›
论文详情
Our official English website, www.x-mol.net, welcomes your feedback! (Note: you will need to create a separate account there.)
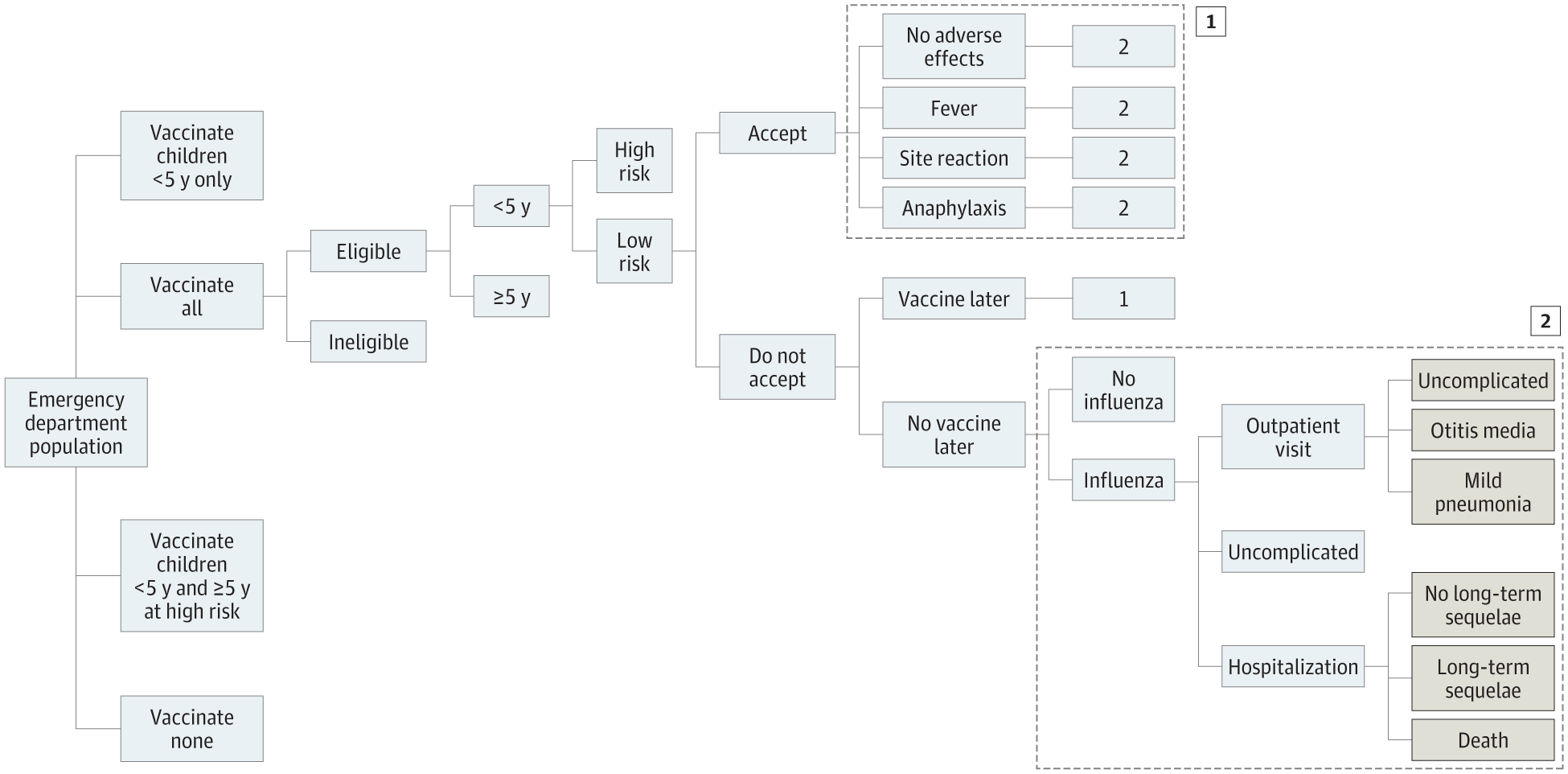
Cost-effectiveness of Strategies for Offering Influenza Vaccine in the Pediatric Emergency Department
JAMA Pediatrics ( IF 26.1 ) Pub Date : 2018-01-02 , DOI: 10.1001/jamapediatrics.2017.3879 Rebecca J. Hart 1 , Michelle D. Stevenson 1 , Michael J. Smith 2 , A. Scott LaJoie 3 , Keith Cross 1
JAMA Pediatrics ( IF 26.1 ) Pub Date : 2018-01-02 , DOI: 10.1001/jamapediatrics.2017.3879 Rebecca J. Hart 1 , Michelle D. Stevenson 1 , Michael J. Smith 2 , A. Scott LaJoie 3 , Keith Cross 1
Affiliation
|
Importance Influenza is a significant public health burden, causing morbidity and mortality in children, yet vaccination rates remain low. Vaccination in the pediatric emergency department (PED) setting may be beneficial but, to date, has not been proven to be cost-effective. Objective To compare the cost-effectiveness of 4 strategies for PED-based influenza vaccine: offering vaccine to all patients, only to patients younger than 5 years, only to high-risk patients (all ages), or to no patients. Design, Setting, and Participants Using commercial decision analysis software, a cost-effectiveness analysis was performed from January 1, 2016, to June 1, 2017, to compare influenza vaccine strategies at a tertiary, urban, freestanding PED with an estimated 60 000 visits per year among a hypothetical cohort of children visiting the above PED during influenza season. Sensitivity analyses estimated the effect of uncertainties across a variety of input variables (eg, influenza prevalence, vaccine price and effectiveness, and costs of complications). Main Outcomes and Measures The primary outcomes were cost and incremental cost-effectiveness ratio in dollars per influenza case averted. Secondary outcomes included total societal costs, hospitalizations and deaths averted, and quality-adjusted life-years gained. Results Offering influenza vaccine to all eligible patients has the lowest cost, at $114.45 (95% CI, $55.48-$245.45) per case of influenza averted. This strategy saves $33.51 (95% CI, $18-$62) per case averted compared with no vaccination, and averages 27 fewer cases of influenza per 1000 patients. Offering vaccine to all patients resulted in 0.72 days (95% CI, 0.18-1.78 days) of quality-adjusted life-years lost, whereas offering to none resulted in 0.91 days (95% CI, 0.25-2.2 days) of quality-adjusted life-years lost. In sensitivity analyses, this strategy remains robustly cost-effective across a wide range of assumptions. In addition to being the most cost-effective strategy regardless of age or risk status, routine vaccination in the PED results in a net societal monetary benefit under many circumstances. In Monte Carlo analysis, offering vaccine to all patients was superior to other strategies in at least 99.8% of cases. Conclusions and Relevance Although few PEDs routinely offer influenza vaccination, doing so appears to be cost-effective, with the potential to significantly reduce the economic (and patient) burden of pediatric influenza.
中文翻译:

在儿科急诊科提供流感疫苗的策略的成本效益
重要性 流感是一项重大的公共卫生负担,会导致儿童发病率和死亡率,但疫苗接种率仍然很低。在儿科急诊科 (PED) 环境中接种疫苗可能是有益的,但迄今为止,尚未证明其具有成本效益。目的比较基于 PED 的流感疫苗 4 种策略的成本效益:向所有患者提供疫苗,仅向 5 岁以下的患者提供疫苗,仅向高危患者(所有年龄)提供疫苗,或不向任何患者提供疫苗。设计、设置和参与者使用商业决策分析软件,从 2016 年 1 月 1 日至 2017 年 6 月 1 日进行了成本效益分析,以比较三级、城市、在流感季节期间访问上述 PED 的假设儿童队列中,估计每年有 60 000 次独立的 PED。敏感性分析估计了各种输入变量(例如流感流行率、疫苗价格和有效性以及并发症成本)的不确定性的影响。主要结果和措施 主要结果是成本和增加的成本效益比(以美元计)避免的每个流感病例。次要结果包括总社会成本、避免的住院和死亡以及获得的质量调整生命年。结果向所有符合条件的患者提供流感疫苗的成本最低,每例避免的流感病例为 114.45 美元(95% CI,55.48-245.45 美元)。与不接种疫苗相比,该策略每避免病例可节省 33.51 美元(95% CI,18-62 美元),每 1000 名患者平均减少 27 例流感病例。向所有患者提供疫苗导致 0.72 天(95% CI,0.18-1.78 天)的质量调整生命年损失,而没有提供疫苗导致 0.91 天(95% CI,0.25-2.2 天)的质量调整生命年生命年损失。在敏感性分析中,该策略在广泛的假设条件下仍然具有强大的成本效益。除了无论年龄或风险状况如何都是最具成本效益的策略之外,PED 中的常规疫苗接种在许多情况下都会产生净社会货币收益。在蒙特卡罗分析中,至少在 99.8% 的病例中,向所有患者提供疫苗优于其他策略。结论和相关性 尽管很少有 PED 常规提供流感疫苗接种,但这样做似乎具有成本效益,
更新日期:2018-01-02
中文翻译:
在儿科急诊科提供流感疫苗的策略的成本效益
重要性 流感是一项重大的公共卫生负担,会导致儿童发病率和死亡率,但疫苗接种率仍然很低。在儿科急诊科 (PED) 环境中接种疫苗可能是有益的,但迄今为止,尚未证明其具有成本效益。目的比较基于 PED 的流感疫苗 4 种策略的成本效益:向所有患者提供疫苗,仅向 5 岁以下的患者提供疫苗,仅向高危患者(所有年龄)提供疫苗,或不向任何患者提供疫苗。设计、设置和参与者使用商业决策分析软件,从 2016 年 1 月 1 日至 2017 年 6 月 1 日进行了成本效益分析,以比较三级、城市、在流感季节期间访问上述 PED 的假设儿童队列中,估计每年有 60 000 次独立的 PED。敏感性分析估计了各种输入变量(例如流感流行率、疫苗价格和有效性以及并发症成本)的不确定性的影响。主要结果和措施 主要结果是成本和增加的成本效益比(以美元计)避免的每个流感病例。次要结果包括总社会成本、避免的住院和死亡以及获得的质量调整生命年。结果向所有符合条件的患者提供流感疫苗的成本最低,每例避免的流感病例为 114.45 美元(95% CI,55.48-245.45 美元)。与不接种疫苗相比,该策略每避免病例可节省 33.51 美元(95% CI,18-62 美元),每 1000 名患者平均减少 27 例流感病例。向所有患者提供疫苗导致 0.72 天(95% CI,0.18-1.78 天)的质量调整生命年损失,而没有提供疫苗导致 0.91 天(95% CI,0.25-2.2 天)的质量调整生命年生命年损失。在敏感性分析中,该策略在广泛的假设条件下仍然具有强大的成本效益。除了无论年龄或风险状况如何都是最具成本效益的策略之外,PED 中的常规疫苗接种在许多情况下都会产生净社会货币收益。在蒙特卡罗分析中,至少在 99.8% 的病例中,向所有患者提供疫苗优于其他策略。结论和相关性 尽管很少有 PED 常规提供流感疫苗接种,但这样做似乎具有成本效益,

























 京公网安备 11010802027423号
京公网安备 11010802027423号