JAMA Oncology ( IF 28.4 ) Pub Date : 2017-09-01 , DOI: 10.1001/jamaoncol.2016.5763 Prashant Kapoor 1 , Stephen M Ansell 1 , Rafael Fonseca 2 , Asher Chanan-Khan 3 , Robert A Kyle 1 , Shaji K Kumar 1 , Joseph R Mikhael 2 , Thomas E Witzig 1 , Michelle Mauermann 4 , Angela Dispenzieri 1 , Sikander Ailawadhi 3 , A Keith Stewart 2 , Martha Q Lacy 1 , Carrie A Thompson 1 , Francis K Buadi 1 , David Dingli 1 , William G Morice 5 , Ronald S Go 1 , Dragan Jevremovic 5 , Taimur Sher 3 , Rebecca L King 5 , Esteban Braggio 2 , Ann Novak 1 , Vivek Roy 3 , Rhett P Ketterling 6 , Patricia T Greipp 6 , Martha Grogan 7 , Ivana N Micallef 1 , P Leif Bergsagel 2 , Joseph P Colgan 1 , Nelson Leung 1, 8 , Wilson I Gonsalves 1 , Yi Lin 1 , David J Inwards 1 , Suzanne R Hayman 1 , Grzegorz S Nowakowski 1 , Patrick B Johnston 1 , Steven J Russell 1 , Svetomir N Markovic 1 , Steven R Zeldenrust 1 , Yi L Hwa 1 , John A Lust 1 , Luis F Porrata 1 , Thomas M Habermann 1 , S Vincent Rajkumar 1 , Morie A Gertz 1 , Craig B Reeder 2
|
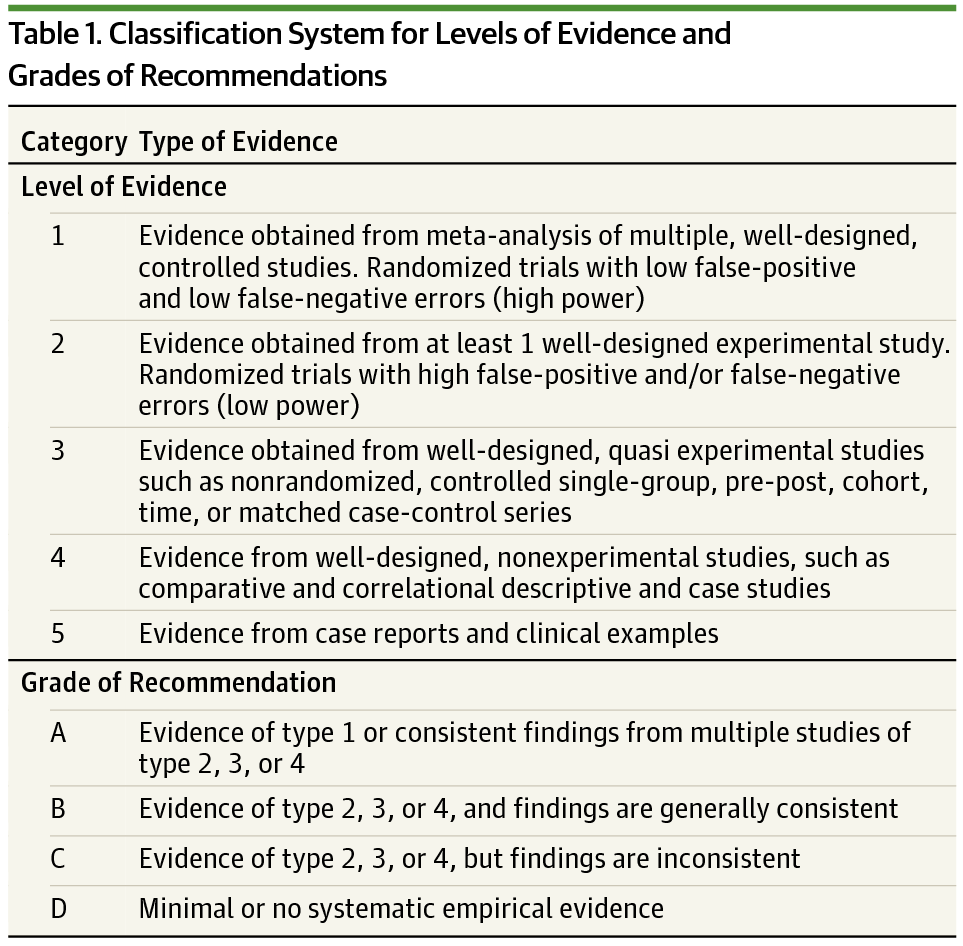
Importance Waldenström macroglobulinemia (WM), an IgM-associated lymphoplasmacytic lymphoma, has witnessed several practice-altering advances in recent years. With availability of a wider array of therapies, the management strategies have become increasingly complex. Our multidisciplinary team appraised studies published or presented up to December 2015 to provide consensus recommendations for a risk-adapted approach to WM, using a grading system.
Observations Waldenström macroglobulinemia remains a rare, incurable cancer, with a heterogeneous disease course. The major classes of effective agents in WM include monoclonal antibodies, alkylating agents, purine analogs, proteasome inhibitors, immunomodulatory drugs, and mammalian target of rapamycin inhibitors. However, the highest-quality evidence from rigorously conducted randomized clinical trials remains scant.
Conclusions and Relevance Recognizing the paucity of data, we advocate participation in clinical trials, if available, at every stage of WM. Specific indications exist for initiation of therapy. Outside clinical trials, based on the synthesis of available evidence, we recommend bendamustine-rituximab as primary therapy for bulky disease, profound hematologic compromise, or constitutional symptoms attributable to WM. Dexamethasone-rituximab-cyclophosphamide is an alternative, particularly for nonbulky WM. Routine rituximab maintenance should be avoided. Plasma exchange should be promptly initiated before cytoreduction for hyperviscosity-related symptoms. Stem cell harvest for future use may be considered in first remission for patients 70 years or younger who are potential candidates for autologous stem cell transplantation. At relapse, retreatment with the original therapy is reasonable in patients with prior durable responses (time to next therapy ≥3 years) and good tolerability to previous regimen. Ibrutinib is efficacious in patients with relapsed or refractory disease harboring MYD88 L265P mutation. In the absence of neuropathy, a bortezomib-rituximab–based option is reasonable for relapsed or refractory disease. In select patients with chemosensitive disease, autologous stem cell transplantation should be considered at first or second relapse. Everolimus and purine analogs are suitable options for refractory or multiply relapsed WM. Our recommendations are periodically updated as new, clinically relevant information emerges.
中文翻译:
Waldenström 巨球蛋白血症的诊断和管理 Mayo 巨球蛋白血症分层和风险适应治疗 (mSMART) 指南 2016
重要性 Waldenström 巨球蛋白血症 (WM) 是一种 IgM 相关的淋巴浆细胞淋巴瘤,近年来见证了一些改变实践的进展。随着更广泛的治疗方法的可用性,管理策略变得越来越复杂。我们的多学科团队评估了截至 2015 年 12 月发表或提交的研究,为使用分级系统的 WM 风险适应方法提供共识建议。
观察 Waldenström 巨球蛋白血症仍然是一种罕见的、无法治愈的癌症,具有异质的病程。WM 中主要的有效药物类别包括单克隆抗体、烷化剂、嘌呤类似物、蛋白酶体抑制剂、免疫调节药物和哺乳动物雷帕霉素靶点抑制剂。然而,来自严格进行的随机临床试验的最高质量证据仍然很少。
结论和相关性 认识到数据的匮乏,我们提倡在 WM 的每个阶段都参与临床试验(如果有的话)。存在开始治疗的特定适应症。在临床试验之外,基于现有证据的综合,我们推荐苯达莫司汀-利妥昔单抗作为大块疾病、严重血液学损害或可归因于 WM 的全身症状的主要治疗方法。地塞米松-利妥昔单抗-环磷酰胺是一种替代方案,特别是对于非大块 WM。应避免常规利妥昔单抗维护。应在细胞减灭术之前立即开始血浆置换,以应对高粘滞症相关症状。对于 70 岁或以下有可能进行自体干细胞移植的患者,可考虑在首次缓解时采集干细胞以备将来使用。复发时,对于既往有持久反应(至下一次治疗的时间≥3 年)且对先前治疗方案耐受性良好的患者,使用原始治疗进行再治疗是合理的。依鲁替尼对患有复发或难治性疾病的患者有效MYD88 L265P 突变。在没有神经病变的情况下,基于硼替佐米-利妥昔单抗的选择对于复发或难治性疾病是合理的。在某些患有化学敏感性疾病的患者中,应在第一次或第二次复发时考虑自体干细胞移植。依维莫司和嘌呤类似物是难治性或多次复发性 WM 的合适选择。随着新的临床相关信息的出现,我们的建议会定期更新。


























 京公网安备 11010802027423号
京公网安备 11010802027423号