当前位置:
X-MOL 学术
›
JAMA Pediatr.
›
论文详情
Our official English website, www.x-mol.net, welcomes your feedback! (Note: you will need to create a separate account there.)
Accuracy of Complete Blood Cell Counts to Identify Febrile Infants 60 Days or Younger With Invasive Bacterial Infections
JAMA Pediatrics ( IF 26.1 ) Pub Date : 2017-11-06 , DOI: 10.1001/jamapediatrics.2017.2927 Andrea T. Cruz 1 , Prashant Mahajan 2 , Bema K. Bonsu 3 , Jonathan E. Bennett 4 , Deborah A. Levine 5 , Elizabeth R. Alpern 6 , Lise E. Nigrovic 7 , Shireen M. Atabaki 8 , Daniel M. Cohen 3 , John M. VanBuren 9 , Octavio Ramilo 10 , Nathan Kuppermann 11 ,
JAMA Pediatrics ( IF 26.1 ) Pub Date : 2017-11-06 , DOI: 10.1001/jamapediatrics.2017.2927 Andrea T. Cruz 1 , Prashant Mahajan 2 , Bema K. Bonsu 3 , Jonathan E. Bennett 4 , Deborah A. Levine 5 , Elizabeth R. Alpern 6 , Lise E. Nigrovic 7 , Shireen M. Atabaki 8 , Daniel M. Cohen 3 , John M. VanBuren 9 , Octavio Ramilo 10 , Nathan Kuppermann 11 ,
Affiliation
|
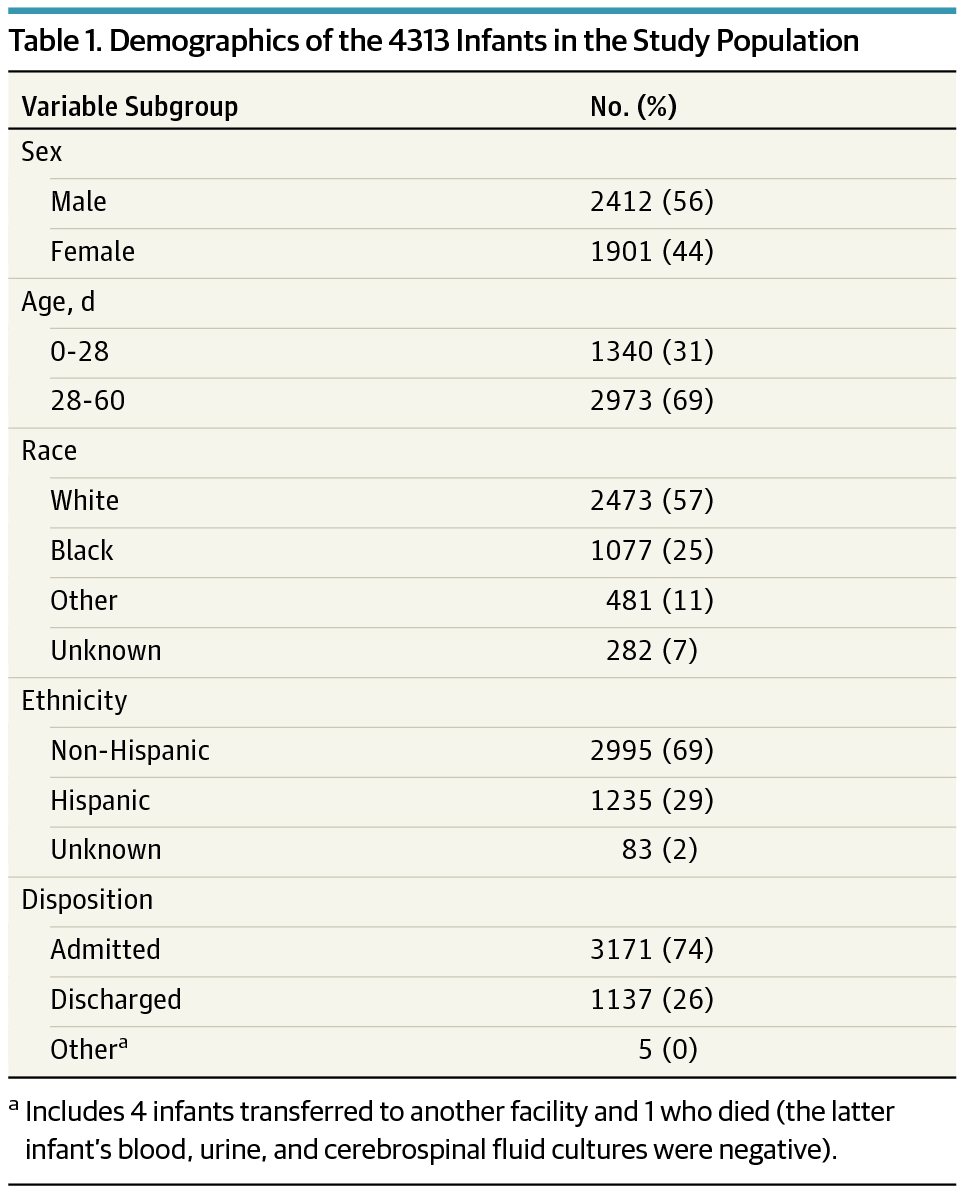
Importance Clinicians often risk stratify young febrile infants for invasive bacterial infections (IBIs), defined as bacteremia and/or bacterial meningitis, using complete blood cell count parameters. Objective To estimate the accuracy of individual complete blood cell count parameters to identify febrile infants with IBIs. Design, Setting, and Participants Planned secondary analysis of a prospective observational cohort study comprising 26 emergency departments in the Pediatric Emergency Care Applied Research Network from 2008 to 2013. We included febrile (≥38°C), previously healthy, full-term infants younger than 60 days for whom blood cultures were obtained. All infants had either cerebrospinal fluid cultures or 7-day follow-up. Main Outcomes and Measures We tested the accuracy of the white blood cell count, absolute neutrophil count, and platelet count at commonly used thresholds for IBIs. We determined optimal thresholds using receiver operating characteristic curves. Results Of 4313 enrolled infants, 1340 (31%; 95% CI, 30% to 32%) were aged 0 to 28 days, 2412 were boys (56%), and 2471 were white (57%). Ninety-seven (2.2%; 95% CI, 1.8% to 2.7%) had IBIs. Sensitivities were low for common complete blood cell count parameter thresholds: white blood cell count less than 5000/µL, 10% (95% CI, 4% to 16%) (to convert to 109 per liter, multiply by 0.001); white blood cell count ≥15 000/µL, 27% (95% CI, 18% to 36%); absolute neutrophil count ≥10 000/µL, 18% (95% CI, 10% to 25%) (to convert to × 109 per liter, multiply by 0.001); and platelets <100 × 103/µL, 7% (95% CI, 2% to 12%) (to convert to × 109 per liter, multiply by 1). Optimal thresholds for white blood cell count (11 600/µL), absolute neutrophil count (4100/µL), and platelet count (362 × 103/µL) were identified in models that had areas under the receiver operating characteristic curves of 0.57 (95% CI, 0.50-0.63), 0.70 (95% CI, 0.64-0.76), and 0.61 (95% CI, 0.55-0.67), respectively. Conclusions and Relevance No complete blood cell count parameter at commonly used or optimal thresholds identified febrile infants 60 days or younger with IBIs with high accuracy. Better diagnostic tools are needed to risk stratify young febrile infants for IBIs.
中文翻译:

全血细胞计数的准确性以识别 60 天或更年轻的有侵袭性细菌感染的发热婴儿
重要性 临床医生经常使用全血细胞计数参数对年轻发热婴儿进行侵袭性细菌感染 (IBIs) 的风险分层,IBIs 定义为菌血症和/或细菌性脑膜炎。目的评估个体全血细胞计数参数的准确性,以识别患有 IBI 的发热婴儿。设计、设置和参与者 对 2008 年至 2013 年儿科急诊应用研究网络中的 26 个急诊科组成的前瞻性观察队列研究进行了计划的二次分析。我们纳入了发热 (≥38°C)、既往健康、年龄更小的足月婴儿超过 60 天的人进行了血培养。所有婴儿都接受了脑脊液培养或 7 天的随访。主要结果与措施 我们测试了白细胞计数、中性粒细胞绝对计数、和 IBI 常用阈值下的血小板计数。我们使用接收者操作特征曲线确定了最佳阈值。结果 在纳入的 4313 名婴儿中,1340 名(31%;95% CI,30% 至 32%)为 0 至 28 天,2412 名为男孩(56%),2471 名为白人(57%)。97 人(2.2%;95% CI,1.8% 至 2.7%)患有 IBI。常见全血细胞计数参数阈值的敏感性较低:白细胞计数低于 5000/µL,10%(95% CI,4% 至 16%)(转换为 109/L,乘以 0.001);白细胞计数 ≥15 000/µL,27%(95% CI,18% 至 36%);中性粒细胞绝对计数 ≥10 000/µL,18%(95% CI,10% 至 25%)(转换为 × 109/L,乘以 0.001);和血小板 <100 × 103/µL,7%(95% CI,2% 至 12%)(转换为 × 109/L,乘以 1)。在受试者操作特征曲线下面积为 0.57 的模型中确定了白细胞计数 (11 600/µL)、绝对中性粒细胞计数 (4100/µL) 和血小板计数 (362 × 103/µL) 的最佳阈值 (95 % CI,0.50-0.63)、0.70(95% CI,0.64-0.76)和 0.61(95% CI,0.55-0.67)。结论和相关性 没有在常用或最佳阈值下的全血细胞计数参数能够以高精度识别 60 天或更年轻的 IBI 发热婴儿。需要更好的诊断工具来对发热的小婴儿进行 IBI 风险分层。结论和相关性 没有在常用或最佳阈值下的全血细胞计数参数能够以高精度识别 60 天或更年轻的 IBI 发热婴儿。需要更好的诊断工具来对发热的小婴儿进行 IBI 风险分层。结论和相关性 没有在常用或最佳阈值下的全血细胞计数参数能够以高精度识别 60 天或更年轻的 IBI 发热婴儿。需要更好的诊断工具来对发热的小婴儿进行 IBI 风险分层。
更新日期:2017-11-06
中文翻译:
全血细胞计数的准确性以识别 60 天或更年轻的有侵袭性细菌感染的发热婴儿
重要性 临床医生经常使用全血细胞计数参数对年轻发热婴儿进行侵袭性细菌感染 (IBIs) 的风险分层,IBIs 定义为菌血症和/或细菌性脑膜炎。目的评估个体全血细胞计数参数的准确性,以识别患有 IBI 的发热婴儿。设计、设置和参与者 对 2008 年至 2013 年儿科急诊应用研究网络中的 26 个急诊科组成的前瞻性观察队列研究进行了计划的二次分析。我们纳入了发热 (≥38°C)、既往健康、年龄更小的足月婴儿超过 60 天的人进行了血培养。所有婴儿都接受了脑脊液培养或 7 天的随访。主要结果与措施 我们测试了白细胞计数、中性粒细胞绝对计数、和 IBI 常用阈值下的血小板计数。我们使用接收者操作特征曲线确定了最佳阈值。结果 在纳入的 4313 名婴儿中,1340 名(31%;95% CI,30% 至 32%)为 0 至 28 天,2412 名为男孩(56%),2471 名为白人(57%)。97 人(2.2%;95% CI,1.8% 至 2.7%)患有 IBI。常见全血细胞计数参数阈值的敏感性较低:白细胞计数低于 5000/µL,10%(95% CI,4% 至 16%)(转换为 109/L,乘以 0.001);白细胞计数 ≥15 000/µL,27%(95% CI,18% 至 36%);中性粒细胞绝对计数 ≥10 000/µL,18%(95% CI,10% 至 25%)(转换为 × 109/L,乘以 0.001);和血小板 <100 × 103/µL,7%(95% CI,2% 至 12%)(转换为 × 109/L,乘以 1)。在受试者操作特征曲线下面积为 0.57 的模型中确定了白细胞计数 (11 600/µL)、绝对中性粒细胞计数 (4100/µL) 和血小板计数 (362 × 103/µL) 的最佳阈值 (95 % CI,0.50-0.63)、0.70(95% CI,0.64-0.76)和 0.61(95% CI,0.55-0.67)。结论和相关性 没有在常用或最佳阈值下的全血细胞计数参数能够以高精度识别 60 天或更年轻的 IBI 发热婴儿。需要更好的诊断工具来对发热的小婴儿进行 IBI 风险分层。结论和相关性 没有在常用或最佳阈值下的全血细胞计数参数能够以高精度识别 60 天或更年轻的 IBI 发热婴儿。需要更好的诊断工具来对发热的小婴儿进行 IBI 风险分层。结论和相关性 没有在常用或最佳阈值下的全血细胞计数参数能够以高精度识别 60 天或更年轻的 IBI 发热婴儿。需要更好的诊断工具来对发热的小婴儿进行 IBI 风险分层。


























 京公网安备 11010802027423号
京公网安备 11010802027423号