当前位置:
X-MOL 学术
›
JAMA Intern. Med.
›
论文详情
Our official English website, www.x-mol.net, welcomes your feedback! (Note: you will need to create a separate account there.)
Association Between More Intensive vs Less Intensive Blood Pressure Lowering and Risk of Mortality in Chronic Kidney Disease Stages 3 to 5
JAMA Internal Medicine ( IF 39.0 ) Pub Date : 2017-10-01 , DOI: 10.1001/jamainternmed.2017.4377 Rakesh Malhotra 1, 2 , Hoang Anh Nguyen 1 , Oscar Benavente 3 , Mihriye Mete 4, 5 , Barbara V Howard 4, 5 , Jonathan Mant 6 , Michelle C Odden 7 , Carmen A Peralta 8 , Alfred K Cheung 9, 10 , Girish N Nadkarni 11 , Ruth L Coleman 12 , Rury R Holman 12 , Alberto Zanchetti 13 , Ruth Peters 14 , Nigel Beckett 15 , Jan A Staessen 16, 17 , Joachim H Ix 1, 18, 19
JAMA Internal Medicine ( IF 39.0 ) Pub Date : 2017-10-01 , DOI: 10.1001/jamainternmed.2017.4377 Rakesh Malhotra 1, 2 , Hoang Anh Nguyen 1 , Oscar Benavente 3 , Mihriye Mete 4, 5 , Barbara V Howard 4, 5 , Jonathan Mant 6 , Michelle C Odden 7 , Carmen A Peralta 8 , Alfred K Cheung 9, 10 , Girish N Nadkarni 11 , Ruth L Coleman 12 , Rury R Holman 12 , Alberto Zanchetti 13 , Ruth Peters 14 , Nigel Beckett 15 , Jan A Staessen 16, 17 , Joachim H Ix 1, 18, 19
Affiliation
|
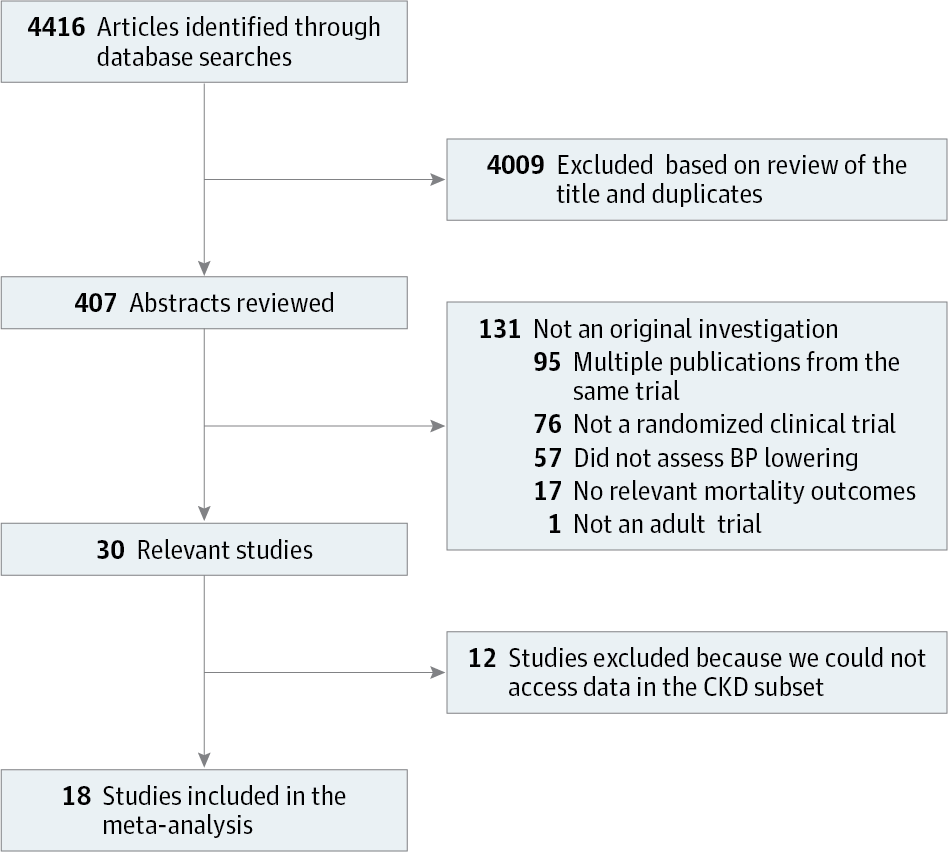
Importance Trials in patients with hypertension have demonstrated that intensive blood pressure (BP) lowering reduces the risk of cardiovascular disease and all-cause mortality but may increase the risk of chronic kidney disease (CKD) incidence and progression. Whether intensive BP lowering is associated with a mortality benefit in patients with prevalent CKD remains unknown. Objectives To conduct a systematic review and meta-analysis of randomized clinical trials (RCTs) to investigate if more intensive compared with less intensive BP control is associated with reduced mortality risk in persons with CKD stages 3 to 5. Data Sources Ovid MEDLINE, Cochrane Library, EMBASE, PubMed, Science Citation Index, Google Scholar, and clinicaltrials.gov electronic databases. Study Selection All RCTs were included that compared 2 defined BP targets (either active BP treatment vs placebo or no treatment, or intensive vs less intensive BP control) and enrolled adults (≥18 years) with CKD stages 3 to 5 (estimated glomerular filtration rate <60 mL/min/1.73 m2) exclusively or that included a CKD subgroup between January 1, 1950, and June 1, 2016. Data Extraction and Synthesis Two of us independently evaluated study quality and extracted characteristics and mortality events among persons with CKD within the intervention phase for each trial. When outcomes within the CKD group had not previously been published, trial investigators were contacted to request data within the CKD subset of their original trials. Main Outcome and Measure All-cause mortality during the active treatment phase of each trial. Results This study identified 30 RCTs that potentially met the inclusion criteria. The CKD subset mortality data were extracted in 18 trials, among which there were 1293 deaths in 15 924 participants with CKD. The mean (SD) baseline systolic BP (SBP) was 148 (16) mm Hg in both the more intensive and less intensive arms. The mean SBP dropped by 16 mm Hg to 132 mm Hg in the more intensive arm and by 8 mm Hg to 140 mm Hg in the less intensive arm. More intensive vs less intensive BP control resulted in 14.0% lower risk of all-cause mortality (odds ratio, 0.86; 95% CI, 0.76-0.97; P = .01), a finding that was without significant heterogeneity and appeared consistent across multiple subgroups. Conclusions and Relevance Randomization to more intensive BP control is associated with lower mortality risk among trial participants with hypertension and CKD. Further studies are required to define absolute BP targets for maximal benefit and minimal harm.
中文翻译:

较高强度与较低强度降压与慢性肾病 3 至 5 期死亡风险之间的关联
重要性 针对高血压患者的试验表明,强化降压 (BP) 可降低心血管疾病和全因死亡率的风险,但可能会增加慢性肾病 (CKD) 的发病和进展风险。强化血压降低是否与流行性 CKD 患者的死亡率获益相关仍不清楚。目的 对随机临床试验 (RCT) 进行系统回顾和荟萃分析,以调查与较低强度的血压控制相比,加强血压控制是否与 CKD 3 至 5 期患者死亡风险降低相关。数据来源 Ovid MEDLINE,Cochrane 图书馆、EMBASE、PubMed、科学引文索引、Google Scholar 和 ClinicalTrials.gov 电子数据库。研究选择 纳入的所有随机对照试验均比较 2 个明确的血压目标(积极血压治疗与安慰剂或不治疗,或强化血压控制与较低强度血压控制),并纳入 CKD 3 至 5 期成人(≥18 岁)(估计肾小球滤过率) <60 mL/min/1.73 m2),仅包含 1950 年 1 月 1 日至 2016 年 6 月 1 日期间的 CKD 亚组。数据提取和合成 我们中的两人独立评估了研究质量,并提取了 CKD 患者的特征和死亡事件每个试验的干预阶段。当 CKD 组的结果之前尚未发表时,我们会联系试验研究人员,索取其原始试验的 CKD 子集内的数据。主要结果和测量各试验积极治疗阶段的全因死亡率。结果 本研究确定了 30 项可能符合纳入标准的随机对照试验。在 18 项试验中提取了 CKD 子集死亡率数据,其中 15 924 名 CKD 参与者中有 1293 人死亡。强度较高组和强度较低组的平均 (SD) 基线收缩压 (SBP) 均为 148 (16) mm Hg。强度较高的组中,平均收缩压下降了 16 毫米汞柱,至 132 毫米汞柱;强度较低的组中,平均收缩压下降了 8 毫米汞柱,至 140 毫米汞柱。加强血压控制与降低血压控制相比,全因死亡率风险降低 14.0%(比值比,0.86;95% CI,0.76-0.97;P = 0.01),这一发现没有显着异质性,并且在多个研究中似乎是一致的。亚组。结论和相关性 随机化进行更强化的血压控制与患有高血压和 CKD 的试验参与者较低的死亡风险相关。需要进一步研究来确定绝对血压目标,以获得最大益处和最小危害。
更新日期:2017-10-01
中文翻译:
较高强度与较低强度降压与慢性肾病 3 至 5 期死亡风险之间的关联
重要性 针对高血压患者的试验表明,强化降压 (BP) 可降低心血管疾病和全因死亡率的风险,但可能会增加慢性肾病 (CKD) 的发病和进展风险。强化血压降低是否与流行性 CKD 患者的死亡率获益相关仍不清楚。目的 对随机临床试验 (RCT) 进行系统回顾和荟萃分析,以调查与较低强度的血压控制相比,加强血压控制是否与 CKD 3 至 5 期患者死亡风险降低相关。数据来源 Ovid MEDLINE,Cochrane 图书馆、EMBASE、PubMed、科学引文索引、Google Scholar 和 ClinicalTrials.gov 电子数据库。研究选择 纳入的所有随机对照试验均比较 2 个明确的血压目标(积极血压治疗与安慰剂或不治疗,或强化血压控制与较低强度血压控制),并纳入 CKD 3 至 5 期成人(≥18 岁)(估计肾小球滤过率) <60 mL/min/1.73 m2),仅包含 1950 年 1 月 1 日至 2016 年 6 月 1 日期间的 CKD 亚组。数据提取和合成 我们中的两人独立评估了研究质量,并提取了 CKD 患者的特征和死亡事件每个试验的干预阶段。当 CKD 组的结果之前尚未发表时,我们会联系试验研究人员,索取其原始试验的 CKD 子集内的数据。主要结果和测量各试验积极治疗阶段的全因死亡率。结果 本研究确定了 30 项可能符合纳入标准的随机对照试验。在 18 项试验中提取了 CKD 子集死亡率数据,其中 15 924 名 CKD 参与者中有 1293 人死亡。强度较高组和强度较低组的平均 (SD) 基线收缩压 (SBP) 均为 148 (16) mm Hg。强度较高的组中,平均收缩压下降了 16 毫米汞柱,至 132 毫米汞柱;强度较低的组中,平均收缩压下降了 8 毫米汞柱,至 140 毫米汞柱。加强血压控制与降低血压控制相比,全因死亡率风险降低 14.0%(比值比,0.86;95% CI,0.76-0.97;P = 0.01),这一发现没有显着异质性,并且在多个研究中似乎是一致的。亚组。结论和相关性 随机化进行更强化的血压控制与患有高血压和 CKD 的试验参与者较低的死亡风险相关。需要进一步研究来确定绝对血压目标,以获得最大益处和最小危害。


























 京公网安备 11010802027423号
京公网安备 11010802027423号