PLOS Medicine ( IF 15.8 ) Pub Date : 2017-07-05 , DOI: 10.1371/journal.pmed.1002322 Belinda J Gabbe 1, 2 , Pam M Simpson 1 , Peter A Cameron 1, 3 , Jennie Ponsford 4, 5 , Ronan A Lyons 1, 2 , Alex Collie 1, 6 , Mark Fitzgerald 7, 8 , Rodney Judson 9 , Warwick J Teague 10, 11, 12 , Sandra Braaf 1 , Andrew Nunn 13 , Shanthi Ameratunga 14 , James E Harrison 15
|
Background
Improved understanding of the quality of survival of patients is crucial in evaluating trauma care, understanding recovery patterns and timeframes, and informing healthcare, social, and disability service provision. We aimed to describe the longer-term health status of seriously injured patients, identify predictors of outcome, and establish recovery trajectories by population characteristics.
Methods and findings
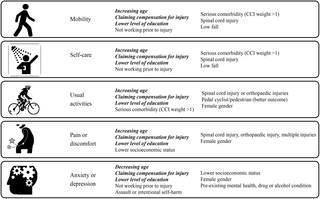
A population-based, prospective cohort study using the Victorian State Trauma Registry (VSTR) was undertaken. We followed up 2,757 adult patients, injured between July 2011 and June 2012, through deaths registry linkage and telephone interview at 6-, 12-, 24-, and 36-months postinjury. The 3-level EuroQol 5 dimensions questionnaire (EQ-5D-3L) was collected, and mixed-effects regression modelling was used to identify predictors of outcome, and recovery trajectories, for the EQ-5D-3L items and summary score. Mean (SD) age of participants was 50.8 (21.6) years, and 72% were male. Twelve percent (n = 333) died during their hospital stay, 8.1% (n = 222) of patients died postdischarge, and 155 (7.0%) were known to have survived to 36-months postinjury but were lost to follow-up at all time points. The prevalence of reporting problems at 36-months postinjury was 37% for mobility, 21% for self-care, 47% for usual activities, 50% for pain/discomfort, and 41% for anxiety/depression. Continued improvement to 36-months postinjury was only present for the usual activities item; the adjusted relative risk (ARR) of reporting problems decreased from 6 to 12 (ARR 0.87, 95% CI: 0.83–0.90), 12 to 24 (ARR 0.94, 95% CI: 0.90–0.98), and 24 to 36 months (ARR 0.95, 95% CI: 0.95–0.99). The risk of reporting problems with pain or discomfort increased from 24- to 36-months postinjury (ARR 1.06, 95% CI: 1.01, 1.12). While loss to follow-up was low, there was responder bias with patients injured in intentional events, younger, and less seriously injured patients less likely to participate; therefore, these patient subgroups were underrepresented in the study findings.
Conclusions
The prevalence of ongoing problems at 3-years postinjury is high, confirming that serious injury is frequently a chronic disorder. These findings have implications for trauma system design. Investment in interventions to reduce the longer-term impact of injuries is needed, and greater investment in primary prevention is needed.
中文翻译:
重伤患者的长期健康状况和轨迹:基于人群的纵向研究
背景
提高对患者生存质量的了解对于评估创伤护理、了解恢复模式和时间框架以及为医疗保健、社会和残疾服务提供提供信息至关重要。我们旨在描述重伤患者的长期健康状况,确定预后的预测因素,并根据人群特征建立康复轨迹。
方法和发现
使用维多利亚州创伤登记处 (VSTR) 进行了一项基于人群的前瞻性队列研究。我们通过死亡登记链接和受伤后 6 个月、12 个月、24 个月和 36 个月的电话采访,对 2011 年 7 月至 2012 年 6 月期间受伤的 2,757 名成年患者进行了随访。收集了 3 级 EuroQol 5 维度问卷 (EQ-5D-3L),并使用混合效应回归模型来确定 EQ-5D-3L 项目和总分的结果预测因子和恢复轨迹。参与者的平均 (SD) 年龄为 50.8 (21.6) 岁,72% 为男性。12% ( n = 333) 在住院期间死亡,8.1% ( n= 222) 的患者在出院后死亡,已知有 155 名 (7.0%) 患者在受伤后存活了 36 个月,但在所有时间点都失访了。受伤后 36 个月报告问题的发生率为 37% 的流动性、21% 的自我护理、47% 的日常活动、50% 的疼痛/不适和 41% 的焦虑/抑郁。受伤后 36 个月的持续改善仅出现在日常活动项目中;报告问题的调整后相对风险 (ARR) 从 6 个月降至 12 个月 (ARR 0.87, 95% CI: 0.83–0.90)、12 个月至 24 个月 (ARR 0.94, 95% CI: 0.90–0.98) 和 24 个月至 36 个月 ( ARR 0.95,95% CI:0.95–0.99)。报告疼痛或不适问题的风险从受伤后 24 个月增加到 36 个月(ARR 1.06, 95% CI: 1.01, 1.12)。虽然失访率很低,在故意事件中受伤的患者、年轻和不太严重的受伤患者不太可能参与,存在反应者偏见;因此,这些患者亚组在研究结果中的代表性不足。
结论
受伤后 3 年持续性问题的发生率很高,这证实了严重的伤害通常是一种慢性疾病。这些发现对创伤系统设计有影响。需要对干预措施进行投资以减少伤害的长期影响,并且需要对初级预防进行更多投资。
























 京公网安备 11010802027423号
京公网安备 11010802027423号